 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
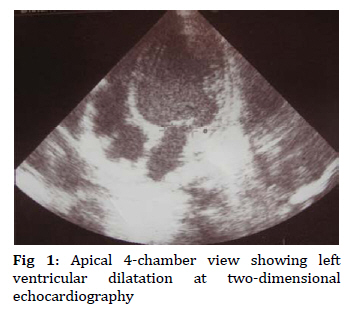
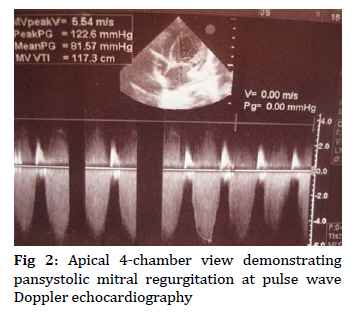
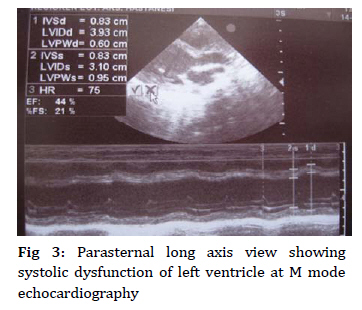
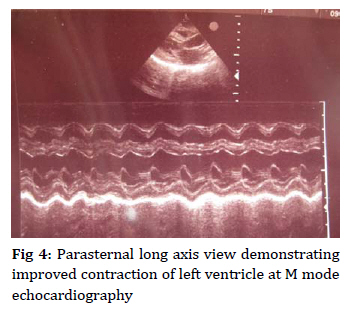
Iranian Journal of Pediatrics, Vol. 19, No. 4, 2009, pp. 413-416 Myocarditis Diagnosed in Twins Osman Ozdemir*1, MD; Samil Hizli2, MD; Ayhan Abaci2, MD1. Department of Pediatric Cardiology, Kecioren Training and Research Hospital, Ankara, Turkey * Corresponding Author; Address: Sanatoryum Caddesi, Pinarbasi Mahallesi, Ardahan Sokak, Kecioren Egitim ve Arastirma Hastanesi, Ankara, Turkey, E-mail: pedkard@gmail.com Received: Mar 04, 2009; Final Revision: May 23, 2009; Accepted: Jun 11, 2009 Code Number: pe09051 Abstract Background: Myocarditis is inflammation of the cardiac myocytes. In the first 6 months of life, myocarditis is slow-progressing and sudden death is common. It should not be forgotten that these patients can have intrauterine myocarditis. Key Words: Congestive heart failure; Myocarditis; Twin Introduction Myocarditis is characterized by inflammatory infiltration of the myocardium with necrosis and/or degeneration of adjacent myocytes not typical of the ischemic damage associated with coronary artery disease. Viral infection agents like adenovirus, coxsackieviruses A and B, echovirus, poliovirus, parvovirus B19 are most common etiologic agents. Other nonviral causes include infectious agents such as rickettsiae, bacteria, protozoa, other parasites, fungi, and yeasts; connective tissue disease; various drugs including antimicrobial medications; hypersensitivity, autoimmune, or collagen-vascular diseases; toxic reactions to infectious agents; or other disorders such as Kawasaki disease and sarcoidosis. However, as etiology cannot be identified in most cases of myocarditis, they are generally considered idiopathic[1,2]. Myocarditis is an underdiagnosed disorder. Clinical findings depend on the age of the child. They may vary from very mild findings to findings of severe cardiac disorder. Nonspecific flulike illness or episodes of gastroenteritis may precede symptoms of congestive heart failure. Patients can be lost suddenly due to arrhythmia, or can heal without sequelae. Clinical progress or prognosis of the disease is affected by genetic features, age, gender, and immune response of the patient and type of the factor. The prognosis of acute myocarditis in newborns and infants is poor, so mortality rate was found very high[1-3]. In this article, 4-month-old twins diagnosed and recovered from myocarditis in a short time with appropriate and supportive therapy in our hospital are presented. Thus, we aim to remind of rare infantile or intrauterine myocarditis. Case Presentation A 4-month-old male patient had fast breathing and cyanosis during crying in the last month. His breath count was 72/minute and O2 saturation was 84%. Subcostal retraction and II/VI pansystolic murmur in the apex were obtained. Examination findings of other systems and first laboratory results were found to be normal. Chest radiogram showed cardiomegaly (heart/ thorax: 0.62). Electrocardiography was normal. Creatine kinase MB (CK-MB), cardiac troponin I (CTI), and N-terminal prohormone brain natriuretic peptide (NT-proBNP) were found 100 mg/dl (normal range: 0-5.6 mg/dl), 2.0 unit (normal range: 0-0.034 unit), and 715 pg/ml (normal range: 0-35.9 pg/ml), respectively. Echocardiography showed dilated left atrium (end-diastolic diameter: 2.7 cm) and dilated left ventricle (end-diastolic diameter: 4.1 cm) at the apical 4-chamber view (Fig 1). At the parasternal long axis view, ejection fraction and shortening fraction of the left ventricle were evaluated as 38% and 18%, respectively. The pansystolic mitral regurgitation (4.78 m/s) was found with the pulse wave Doppler imaging at the apical 4-chamber view (Fig 2). Thus, the patient was diagnosed with myocarditis. As the patient had a twin brother, we decided to evaluate the second baby too. The findings of physical examination of the twin brother were normal except for hypoxia (O2 saturation 89%). Creatine kinase MB, CTI, and NT-proBNP of the second patient were found 55 mg/dl, 0.05 unit, and 95 pg/ml, respectively. In his echocardiographic examination at the parasternal long axis view, ejection fraction and shortening fraction of the left ventricle were evaluated as 44% and 21%, respectively (Fig 3). Infectious and metabolic scanning tests were performed on both patients. No underlying viral cause was found. Enteroviral and adenoviral antibody titers, Epstein-Barr virus, cytomegalo- virus, and human immunodeficiency virus were negative. Lactic acid and pyruvic acid of blood, the amino acids of urine and blood, the organic acid of urine, and the tandem mass spectrometry of blood were normal in the twins. Antinuclear antibody (ANA), rheumatoid factor (RF), and anti-doublestrain deoxyribonucleic acid (anti-ds DNA) were negative in the patients and their mother. The symptoms and findings of the patients were treated in two weeks. At echocardiographic control, ventricles, atria and left ventricle functions of the patients became normal by the end of 6 weeks (Fig 4). Discussion Clinical findings of myocarditis depend on the age of the child. Sudden death may occur in some infants with myocarditis, or following a few days of non-specific complaints in others. Poor appetite, anorexia, fever or hypothermia, irritability or listlessness, periodic episodes of pallor, and diaphoresis are seen. On physical examination, pallor and mild cyanosis in addition to classic symptoms of congestive heart failure are commonly noted[1,2,3]. The younger the child, the more likely it is that intrauterine myocarditis is taken for a chronic disease. Sepsis, hypoxia, hypoglycemia, hypocalcemia, structural heart disease, idiopathic dilated cardiomyopathy, Barth syndrome, endocardial fibroelastosis, anomalous left coronary artery originated from the pulmonary artery, and cerebral arterio-venous malformation should be eliminated in the newborns and infants because of similarity of clinical findings[1]. Because of the symptoms and findings of our patient, we suspected congestive heart failure. CK-MB, troponin-I and NT- proBNP tests were found too high. Cardiomegaly was found on chest radiogram. Not only dilatation of left ventricle and left atrium without any structural heart disease, but also mitral regurgitation resulting from the dilatation were found on echocardiography (Fig 1 and 2). So, myocarditis was diagnosed in the patient due to unexplained congestive heart failure. Differential diagnosis was made with the help of further studies. Possible other diagnoses were eliminated by making the same studies on the later-diagnosed asymptomatic twin. Viral culture of blood, as done in our patients, is commonly performed but is unreliable at identifying the causative infection. The other appropriate diagnostic study of myocarditis is endomyocardial biopsy from the right ventricle [1,2]. However, endomyocardial biopsy was not taken as the presented patients were very young with severe ventricular dilatation, and their clinics improved fast. As a result, they are considered to have early-stage myocarditis. Prognosis of myocarditis in children gets worse with decreasing age. Myocarditis is especially slow-progressing in newborns and infants, and sudden death is common. Mortality in myocarditis cases identified in older children is reported as 10-25%. However, this rate is considered to be much higher in infants. Most deaths occur in the first week of the disease[3]. The anticongestive treatment and the supportive therapy, such as oxygen, digital, furosemide, enalapril, acetyl salicylic acid, were given to the patients. Complete healing was seen in a short time without any arrhythmia. Chronic arrhythmias may persist long after the acute myocarditis has passed. Thus, children who recover from myocarditis, regardless of cause, should be followed indefinitely[1-3]. Therefore, our patients have been followed for 18 months and no arrhythmia has been found. Enteroviral infections late in pregnancy are common, especially during periods of high prevalence of community infection. Most of these infections, however, are not associated with significant maternal or neonatal disease. Conversely, 65% of women who gave birth to infants with proven enteroviral infection had symptomatic disease during the perinatal period. Transmission of enteroviruses from mother to infant may occur through contact with maternal secretions during vaginal delivery, blood, or upper respiratory tract secretions. Intrauterine transmission has been documented, but its frequency is unknown[4]. Coxsackievirus intrauterine infection has been documented mostly on the basis of indirect evidence of transplacental transmission[5,6]. Neonatal disease may range from asymptomatic infection to overwhelming systemic illness and death. Common clinical syndromes associated with neonatal enteroviral infections are meningoencephalitis, pneumonia, myocarditis, hepatitis, and generalized sepsis[4-6]. The severity and outcome of perinatally acquired enteroviral infection is influenced by several factors, including the virus strain involved, mode of transmission, and presence of passively acquired serotype-specific maternal antibody [4]. Parvovirus B19 infection during pregnancy is at risk of adverse fetal outcome. The risk is increased if maternal infection occurs during the first two trimesters, but may also happen during the third trimester[7]. Infection during pregnancy can cause severe fetal anemia, neurological anomalies, nonimmune hydrops fetalis, and fetal death[7,8]. Parvovirus B19 infection during pregnancy causes up to 27% cases of non-immune hydrops in anatomically normal fetuses[8]. Cardiac tropism of the virus can cause myocarditis and aggravate the cardiac failure. Myocarditis leading to heart failure may contribute to the development of fetal hydrops[7]. Conclusion Myocarditis, seen in the first 6 months of life, is slow-progressing and sudden death is common. It should not be forgotten that these patients can have intrauterine myocarditis. Even though no etiologic agent can be assigned to our patients, we think that the twins have intrauterine myocarditis due to similar findings and recovering periods. References
© Copyright 2009 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe09051f2.jpg] [pe09051f4.jpg] [pe09051f1.jpg] [pe09051f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}