 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
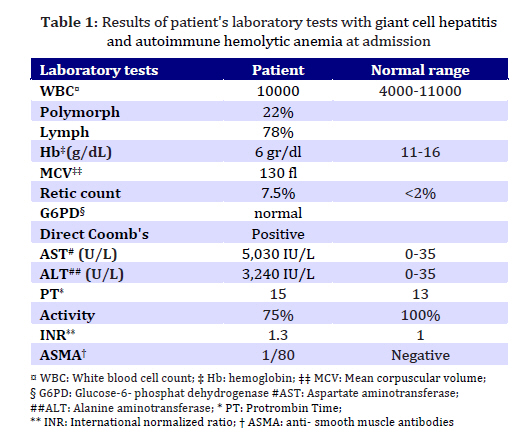
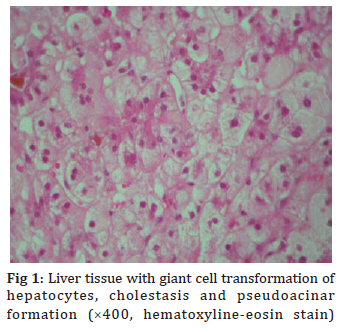
Iranian Journal of Pediatrics, Vol. 19, No. 4, 2009, pp. 421-424 Giant Cell Hepatitis with Autoimmune Hemolytic Anemia; a Case Report Mehri Najafi1, MD; Vajiheh Modarresi1, MD; Kambiz Eftekhari1, MD; Fatemeh Mahjoub2, MD; Mina Izadyar1, MD 1. Department of Pediatrics, Childrenۥs Medical Center, Pediatrics Center of Excellence, Tehran University of Medical Sciences, Tehran, IR Iran * Corresponding Author; Address: Gastroenterology Division, Childrenۥ s Medical Center, Dr.Gharib St, Keshavarz Blvd, Tehran, IR Iran, Email: drmodarressi@gmail.com Received: Jan 30, 2009; Final Revision: Apr 25, 2009; Accepted: May 22, 2009 Code Number: pe09053 Abstract Background: Giant cell hepatitis (GCH) is a histological finding in infants with neonatal cholestasis and rarely can be seen after this period. Autoimmune hemolytic anemia (AIHA) which is characterized by massive and acute red blood cell destruction due to antibody production, responds favorably to corticosteroid therapy. The combination of GCH and AIHA is a rare distinct entity that carries poor response to immunosuppressive therapy and often progresses to fatal liver disease. Key Words: Giant cell hepatitis; Autoimmunity; Hemolytic anemia; Rituximab Introduction Giant cell hepatitis (GCH) is a common histological finding in infants with neonatal cholestasis and is rare after this period. Important known risk factors for GCH are viral infections, drugs, and autoimmune disorders, but in most cases the etiology could not be found [1].Although GCH and Autoimmune hemolytic anemia (AIHA) are two distinct entities that may occur in neonatal period separately, in a very rare condition they can involve one case simultaneously. Because of liver dysfunction, despite immunosuppressive therapy the disease progresses to fatal outcome. Positive direct Coombs test and anti- smooth muscle antibodies (ASMA) and Anti mitochondrial antibody (AMA) are the signs of autoimmunity in these patients[2]. Presentation of the disease usually begins with anemia that can be proved as autoimmune by positive direct Coombs test. These patients are initially diagnosed with isolated AIHA. Hepatitis may have the same presentation as viral hepatitis with similar signs, symptoms, and laboratory findings, but more commonly, it has an insidious onset over several weeks or months[3]. It is supposed the mechanism of liver disease to be autoimmune. The liver dysfunction would have a rapidly progressive and fatal course if therapeutic intervention is not sufficient. Early recognition of the disease and prompt institution of immunosuppressive therapy results in clinical remission and prevents liver disease progression. Common therapeutic regimen is combination of steroids and azathioprine or cyclosporine[1,8,9].Early initiation of steroids has been shown to have a beneficial effect for both liver function and autoimmune hemolytic anemia. Steroids have been demonstrated to significantly reduce the mortality in the early active phase[4]. Since, this condition is rare, there is few experience in treatment of refractory cases and most of suggested therapeutic regimens are based on individual experience[1,8,9]. We report on an infant with GCH and AIHA whose hemolytic process failed to respond to steroids, azathioprine, cyclosporine, and intravenous immunoglobulin (IVIG) but improved clinically and biochemicaly after 4 courses of rituximub, a CD20 monoclonal antibody. Case Presentation A 13-month-old boy presented with acute onset of jaundice and anemia following an upper respiratory tract infection. There were no complains of acholic stool, fever, weight loss and gastrointestinal bleeding. He was first child from unrelated parents. The patient had no history of Glucose-6- phosphat dehydrogenase (G6PD) deficiency and liver disease or neonatal jaundice. In physical examination he had pale mucosae and icteric sclerae. His height and weight were at the 50th percentiles for his age. Vital signs were stable and heart and lungs were normal. Left lobe of liver was palpable and splenomegaly was detected (5 cm under the sub costal margin). No lymphadenophaty was detectable. Early onset of digital clubbing, but no palmar erythema was observed in extremities. Blood tests revealed severe anemia and abnormal liver function test as shown in table 1. In urine analysis bilirubin, urobilinogen and blood was detected. Serologic evaluation was negative for hepatitis viruses A, B, and C, Epstein-Barr virus, Cytomegalovirus and HIV.Abdominal sonography revealed splenomegaly, but liver had normal size and homogenous echogenicity. No ascites. Liver biopsy showed giant cell transformation of hepatocytes with modrate inflammation and mild interface hepatitis. A moderate portal fibrosis (stage 3, Hepatic activity index) was also evident (Fig. 1). Wright's stained bone marrow aspirate showed relatively normal distribution of both erythroid and myeloid precursors. Based on clinical manifestations, biochemical tests and pathologic report, and consultation with hematologist, the diagnosis of GCH with AIHA was considered. Treatment started with IV infusion of IVIG (1 gr/kg /day) and methyl prednisone (10 mg/kg/day) for three days, followed by prednisone (2 mg/kg/day) orally. Hemoglobin level increased and liver enzyme level decreased (Hb=14, ALT=264, AST=124). Prednisone was tapered after 4 weeks; this led to increased liver enzyme level. The dose of prednisone was increased again to 4mg/kg/day, and azathioprine (1.5 mg/ kg/day) added, but no response was observed, and liver enzyme level was continuously increasing (AST=1,290, ALT=1,990). We added cyclosporine (5mg/kg/day). This combination of drugs induced partial response and liver enzyme level decreased slowly and reached normal range within 2 years, ultimately. Unfortunately anemia relapsed and did not respond to corticosteroid and immunosup-pressants; this time rituximab (375 mg/m²/wk) was given for a total of 4 doses. Its effective results in refractory cases are reported by other authors[1]. It was well tolerated and resulted in significant improvement without any adverse effects. Prednisone and other immunesuppressive drugs were tapered gradually. Fortunately the patient did not show any sings of either GCH or AIHA in later visits. Now he is 6 years old and in a fairly good condition. Discussion The association of AIHA with GCH is an uncommon condition that can be life threatening usually leading to hepatic failure and death. This condition is a rare variation of more common GCH in the neonatal period, in association with infections, metabolic disorders, and cholestasis[1]. Although it can be cured by immunosuppressive agents, no direct evidence exists for an autoimmune pathogenesis. Autoantibodies are usually negative and histological characteristics of autoimmune hepatitis are not seen. There have been 20 reported cases of GCH with AIHA[5]. Disease onset in all of the patients occurred between 4 and 24 months of life. Also our patient presented as he was 13 months old. The clinical course usually begins with AIHA and GCH follows; the hepatitis presents more insidiously[9]. In our case both entities started simultaneously and AIHA had more aggressive course. Most patients initially respond to immunosuppressants[4], but usually relapse to have poor outcome. Our patient had more serious problem with AIHA. Liver involvement responded to common treatment but AIHA progressed to fatal condition. Usual immunosuppressive therapy includes steroids, azathioprine, cyclosporine A, tacrolimus, mycophenolate mofetil, sirolimus, vincristine, IVIG, and plasmapheresis with varying degrees of benefit[1,6]. The GCH associated with AIHA specifically is believed to have a unique and different etiology from typical neonatal GCH. An autoimmune component has been suggested due to the associated Coombs-positive AIHA. Rituximab, an anti-CD 20 monoclonal antibody, inhibits B cell proliferation and prevents further antibody production. It has been effectively used in chronic refractory AIHA[7]. In our patient the liver disease responded ultimately to steroids and immunosuppressive therapy (AZA and cyclosporine) after 1.5-2 years. AIHA recurred, while liver function tests were normal, and it had no response to high doses of corticosteroid. Rituximab (375mg/m²/wk) was used as rescue therapy and resulted in dramatic improvement, without any significant side effects. Now he is in good condition with normal liver function tests and Hb (11 gr/dl). Conclusion The combination of GCH with AIHA is an uncommon condition with poor prognosis in infancy. Most patients initially respond to immunosuppressants but usually relapse to have an aggressive course. In our case, liver function became normal with combination of prednisolone and azathioprin and then cyclosporine therapy; however, the AIHA was refractory to steroids, azathioprine, cyclosporine and IVIG. Since rituximab therapy led to improvement of AIHA, we conclude that it should be considered as a rescue therapy of refractory cases of GCH with AIHA. References
© Copyright 2009 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe09053f1.jpg] [pe09053t1.jpg] |
| |||||||||

{kind=link}
{kind=link}