 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
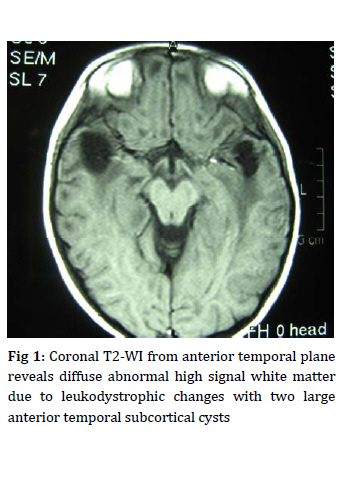
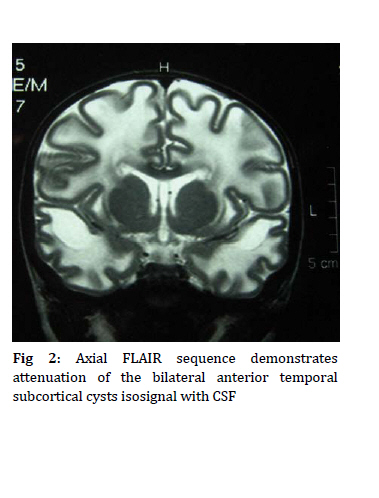
Iranian Journal of Pediatrics, Vol. 19, No. 4, 2009, pp. 425-429 A Case of Megalencephalic Leukoencephalopathy with Subcortical Cysts in an Iranian Consanguineous Family Mahmoud Reza Ashrafi1, MD; Ariana Kariminejad*2, MD; Houman Alizadeh1, MD; Bita Bozorgmehr2, MD; Sepideh Amoeian1, MD; Mohammad-Hasan Kariminejad2, MD 1. Department of Pediatrics, Children's Medical Center, Pediatrics Center of Excellence, Tehran University of Medical Sciences, Tehran, IR Iran * Corresponding Author; Address: Kariminejad Najmabadi Pathology and Genetics Center, 1143 Med Bldg, Sanat Sq, Shahrak Gharb, Tehran, IR Iran, E-mail: arianakariminejad@yahoo.com Received: Nov 10, 2008; Final Revision: Mar 17, 2009; Accepted: May 25, 2009 Abstract Background: Megalencephalic leukoencephalopathy with subcortical cysts (MLC) is an autosomal recessive disorder characterized by macrocephaly, and slowly progressive clinical course marked by ataxia, spasticity and mental decline. MLC is caused by mutations in the gene MLC1 which encodes a novel protein, MLC1. Key Words: Macrocephaly; Leukoencephalopathy; Megalencephaly; MLC1 gene Introduction Megalencephalic leukoencephalopathy with subcortical cysts (MLC) is a recently described autosomal recessive disease[1-4]. The clinical features consist of macrocephaly occurring at birth or, much more commonly, in the first year of life with a delayed onset of relatively mild neurologic abnormalities, consisting of cerebellar ataxia, pyramidal tract signs and seizures. Brain MRI is characterized by diffuse supratentorial white matter increased signal on T2-weighted images, decreased signal on T1-weighted images with cysts in the subcortical temporal and often parietal region, with relative sparing of central structures, brain stem and cerebellum. Mutations in the MLC1 gene have been identified in 80% of MLC patients. MLC has been diagnosed in many ethnic groups (Turkish, Indian, Pakistani, Croatian, Portuguese, Brazilian, Japanese, US Americans), however this is the first report in an Iranian family. Case Presentation The propositus is a four and a half-year-old female, the first and only child of first cousins once removed. Pregnancy was uneventful. She was born at term by cesarean section due to oligohydramnios detected by sonography. Birth weight, length and head circumference were 3,200 grams, 51 cm and 36 cm respectively. At 4 months of age she was seen for macrocephaly. Her developmental milestones were normal in the first year of life. Head control was possible at 3 months, sitting without support at 8 months and independent walking at 13 months of age. She smiled socially between 2-3 months of age and said her first words at 17 months. Her parents said that she experienced frequent falls on the back, and in one time with transient loss of consciousness. She was hospitalized at this incident however the reason for her loss of consciousness was not determined. First visit at the age of 2 years showed macrocephaly, head circumference 55 cm [>98th centile], and normal development. Except for slight increase of valine in blood amino acid chromatography with High Performance Liquid Chromatography (HPLC) method, other metabolic laboratory examinations including arterial blood gas parameters, blood lactate, and ammonia and urine amino acid chromatography were normal. Creatine phosphokinase (CPK) was within normal limit. Brain Computerized Tomography (CT) scan showed diffuse white matter diminished attenuation. Brain MRI showed diffusely abnormal cerebral white matter with a high signal on T2-weighted sequences (Fig 1). It also revealed large bilateral anterior temporal and smaller subcortical cysts in the frontal regions, isointense with cerebrospinal fluid on all sequences (Fig 2). Central white matter was relatively better preserved. Electroencephalography (EEG) was normal. Patient was re-examined at age 4. Physical examination revealed head circumference of 57cm (>98th centile), weight 20 kg (>75th centile), length 110 cm (90th centile). Mild cerebellar ataxia and lower limb spasticity were found without tremor or nystagmus. She was attending kindergarten with other children of the same age. Her instructor says that she is doing relatively well but memorizing verses is more difficult for her than for her classmates or that her drawings are not at the same level as her classmates. Chromosomal analysis revealed normal 46,XX pattern. Sequence analysis of the MLC1 gene revealed a homozygous mutation c.177+1g>T, which leads to a splicing defect at protein level and probably to a deletion of part of the protein. Both parents were heterozygous for this mutation. Discussion Megalencephalic leukoencephalopathy with subcortical cysts (MIM 604004) was first described by van der Knaap et al, in 1995[1]. MLC is an autosomal recessive disorder due to mutations in MLC1 gene[5,6,7]. In many reported cases the parents were related[2,3,4,8-11]. Macrocephaly has been identified in all reported cases to date. Macrocephaly usually develops within the first year of life, but is present at birth in exceptional cases[8,12,13,14] Macrocephaly develops during the first 6 months in 24% of patients and 70% in the second six months. In this respect our patient had early onset of macrocephaly, before 6 months of age. The main presenting features after macrocephaly are pyramidal findings and ataxia which are age dependent. Spasticity and ataxia usually develop by 5 years of age and are usually slowly progressive. Loss of independent ambulation was seen in 38% of reported patients and occurred at an average age of 7.2 years. In all patients, early psychomotor development is normal, as was in our patient[12,13] or mildly delayed[8,14]. Most patients can walk independently but slow deterioration of motor function with cerebellar ataxia and spasticity usually starts in early childhood. The clinical course is relatively mild. Our patient can still walk independently and shows slow deterioration of motor function with ataxia and spasticity starting at age 4. Seizures, extrapyramidal movement abnormalities with dystonia or athetosis are described in some patients as late findings. Mental decline occurs later and is much milder than motor decline. Our patient presented with macrocephaly, slowly progressive neurologic deterioration, mild ataxia and spasticity. There have been reports of mental and motor deterioration and loss of consciousness, that may follow infection or minor head trauma[1,3,10,11,14,15,16]. This patient had no definite history of seizure disorders, but one episode of loss of consciousness following a mild head trauma. Brain MRI findings were more serious than that of the clinical picture[1,2] and consisted of characteristic diffuse supratentorial white matter increased signal intensity on T2-weighted images, decreased signal intensity on T1-weighted images, mild swelling of the abnormal white matter and subcortical cysts of temporal, parietal and frontal regions. The differential diagnosis of MLC includes Canavan's disease, Alexander disease, infantile onset GM2, GM1 gangliosidosis, glutaric aciduria and merosin deficient congenital muscular dystrophy. MLC characteristically has an early onset and slow progression whereas Canavan and Alexander's disease have a more rapid progression and neurological deterioration is severe so that the patients have spasticity and seizures from a young age. Glutaric aciduria was ruled out biochemically. Absence of muscle weakness and normal CPK ruled out congenital muscular dystrophy. In Canavan's disease, involvement of the globus pallidus and the thalamus is seen, which are spared in MLC[17] also absent in our patient. Although cystic white matter may be seen in Canavan's disease, the typical subcortical cyst is lacking. Alexander's disease leads to a magalencephaly and leukoencephalopathy with frontal predominance, sometimes hydrocephalus, cavitation and cystic degeneration in the frontal deep white matter[8,18] and abnormal enhancement of caudate nuclei, anterior columns of the fornices and periventricular areas. These findings were absent in our patient MRI in infantile GM2 gangliosidosis shows prominent involvement of the basal ganglia and thalami in addition to the white matter abnormalities. MRI feature in infantile GM1 gangliosidosis are very similar to those of GM2 gangliosidosis[19]. This disease has been successfully diagnosed prenatally [20]. Conclusion In conclusion we believe that our neurologists should be more aware of this disease, since as in all genetic disease transmitted in an autosomal recessive manner, the risk increases in regions with high prevalence of consanguineous marriages, such as ours. However, by appropriate action, diagnosis and molecular testing of the MLC 1 gene, we will be able to offer prenatal diagnosis. Acknowledgment We thank Dr. Marjo S. van der Knaap and Dr. Gert C. Scheper, Amsterdam, The Netherlands, for performing analysis of the MLC1 gene. References
© Copyright 2009 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe09054f2.jpg] [pe09054f1.jpg] |
| |||||||||

{kind=link}
{kind=link}