 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 19, No. 4, 2009, pp. 430-434 Paratesticular Embryonal Rhabdomyosarcoma; Report of a Case Sefa Resim1, MD; Nazan Okur2, MD; Sevgi Bakarıs3,MD; Ali Osman Kilic1, MD; Bulent Altunoluk1, MD 1. Department of Urology, KSU Faculty of Medicine, Kahramanmaras, Turkey * Corresponding author; Address: Haydarbey mah Karasu Bulvarı, Yeşilkent Sitesi C blok, Kat 6, Daire 27, 46050 Kahramanmaraş, Turkey, E-mail: sresim@yahoo.com Received: Nov 12, 2008; Final Revision: Dec 23, 2008; Accepted: Jan 25, 2009 Code Number: pe09055 Abstract Background: Paratesticular rhabdomyosarcoma is the most common pediatric soft-tissue sarcoma, often presenting in the first two decades after birth. Paratesticular embryonal rhabdomyosarcoma (RMS) is a rare tumor arising from the mesenchymal tissues of the spermatic cord, epididymis, testis and testicular tunics. It represents only 7% of all patients entered in the Intergroup Rhabdomyosarcoma Study (IRS) and 17% of all malignant intrascrotal tumors in children less than 15 years old. Key Words: Paratesticular embryonal rhabdomyosarcoma; Testis; Tumor; Adolescent
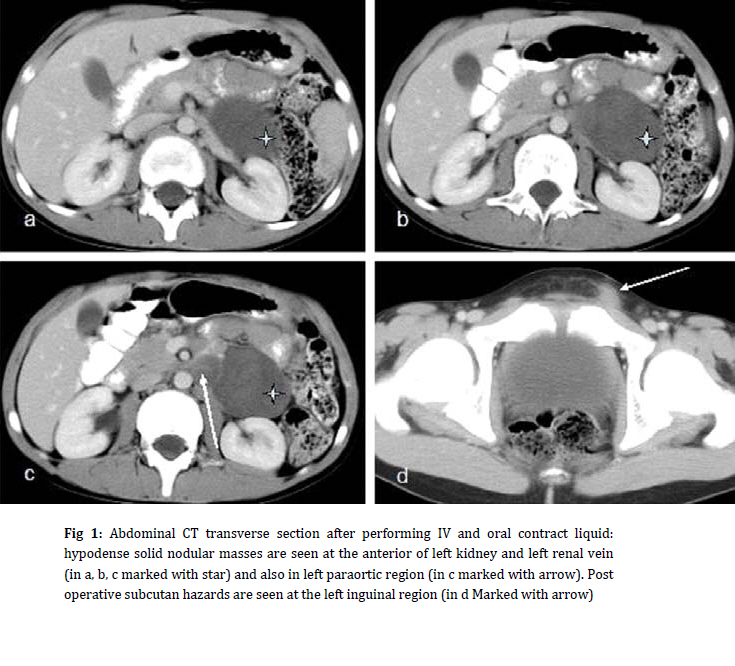
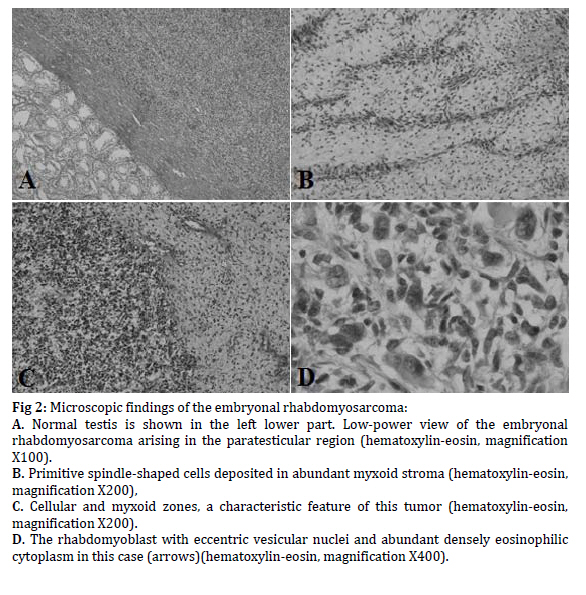
Introduction Testicular and paratesticular tumors in children are rare. Seven to 10% of primary genitourinary tumors locate in paratesticular region. Scrotal rhabdomyosarcomas generally originating from paratesticular tissue are most frequently seen in childhood and young adulthood[1]. Paratesticular rhabdomyosarcomas typically present as a unilateral, painless scrotal swelling or mass above the testis. Lymph node metastasis develops in approximately one-third of cases with paratesticular lesions[2]. Hematogenous metastases to lungs, liver, bone and bone marrow is present in 20% of patients at initial presentation[3]. In some conditions, testicular and/or paratesticular masses were given different diagnoses such as inguinal hernia, hydrocele[4], especially if the scrotal ultrasonography was not performed. We report a boy with paratesticular embryonal rhabdomyosarcoma, who underwent inguinal surgery misdiagnosed as being inguinal hernia. He survives without recurrences for 15 months after management with multidisciplinary approach. Case Presentation A 14-year-old boy presented to clinic of general surgery in an urban state hospital with a 2- month history of testicular swelling and a painless mass in the left scrotum. The patient was planned to be operated for inguinal hernia by a general surgeon after physical examination. During operation, the surgeon realized that the mass was not an inguinal hernia, it seemed like a testicular tumor and then a urologist was consulted. The patient underwent left high inguinal orchiectomy. The testis and epididymis were tumor-free. The tumor was localized in paratesticular area (Fig. 1). On histopatho-logical examination, the removed solid mass was completely encapsulated and measured nearly 4.5×3.5× 2.5 cm. The tumor was covered by normal testis tissue (Fig. 1A) and composed of oval to spindle cells with vesicular nuclei. In most areas, there was abundant intercellular myxoid material with few inflammatory cells (Fig. 1B). Few cellular areas with fascicular arrangement were seen. In some areas, the tumor cells had varying degrees of cellularity with alternating densely packed hypercellular areas and loosely textured myxoid areas (Fig. 1C). Mitotic figures were frequently observed. There was pleomorphism. Many multinucleated cells were also observed, however, strap cells were not observed (Fig. 1D). The tumor cells were positive for desmin while negative for alpha-smooth-muscle actin on immunohistochemistry. In addition, hemorrhage, necrosis and infiltration of the lymphocytes and plasma cells were also focally observed. Final pathological diagnosis was paratesticular embryonal rhabdomyosarcoma. The patient was referred to our clinic for further investigation. The other testicle was normal in physical examination. His serum markers for α-fetoprotein, β-human chorionic gonadotropin and lactate dehydrogenase were normal. CBC and ESR levels were normal. The radiography and computed tomogram of chest was normal. Post-operative computed tomogram of the abdomen and pelvis showed a sharp limited mass with the dimensions of 6,5x5x4 cm which had a visual density of soft tissue placed in front of the left kidney and extending from tale of pancreas to inferior pole of the kidney (Fig. 2). Another mass measuring 25X23 mm with similar density was seen medial to the big mass stated earlier. These were interpreted as retroperitoneal lymph node masses. There were minimal lymph node masses in para-aortic space and mesenteric adipose tissue as well (Fig. 1). The patient was diagnosed as having paratesticular embryonal rhabdomyo-sarcoma with retroperitoneal lymph node mass. We referred him to the oncology department. The patient was followed up post-operatively with chemotherapy. Vincristine, doxorubicin and cyclophos-phamide (VAC) regimen was used. The patient is disease-free in follow-up 15 months after completion of chemotherapy.Discussion Paratesticular rhabdomyosarcomas, which consist 7% of all rhabdomysarcomas, are rare tumors. The painless mass lesion originating from spermatic cord, epididymis, or testicular envelopes is diagnosed generally early, and is removed with radical surgery[1,5]. Paratesticular rhabdomyosarcomas are treated with combined treatment protocols. These protocols include inguinal radical orchiectomy, local radiotherapy to eliminate microscopic and macroscopic residual tumors, and multiple chemotherapy protocols[6]. Five-year survivals are reported to be over 80% with these treatment protocols[6,7]. Paratesticular rhabdomyosarcoma still represents the most common non-germinal malignant tumor in this site[8]. The peak incidence is between 1 to 5 years of age[9]. Embryonal rhabdomyosarcoma is the predominant histological subtype in 90% of paratesticular rhabdomyosarcomas and has a good prognosis. Embryonal rhabdomyosarcoma is the most common subtype observed in children, accounting for approximately 60% of all cases in this age group[6]. The clinical presentation tends to include a short history, usually only a few weeks of painless swelling of the scrotum occurring most often in a child or an adult under 21 years. The tumor has no preference for the left or right testis or for any particular race. Spread of the tumor is mostly by lymphatics to the iliac and para-aortic nodes, but haematogenous spread does occur, most commonly to the lungs and liver. It spreads via lymphatics earlier than by haematogenous spread[7,8]. One-third of patients already have metastases at the time of presentation as in our case. The management of this disease has dramatically changed over the years, and today the emphasis is on a multidisciplinary approach. Before 1960, while survivals of localized rhabdomyosarcomas treated with either surgery or radiation therapy were less than 30%, today, the survival rates elevated to 90% with chemotherapy regimens in combination with surgery or radiation therapy[9,10]. The typical patient presentation for paratesticular rhabdomyosarcoma is a painless scrotal mass. Our patient presented with a 2- month history of testicular swelling and a painless mass in the left scrotum. As occurred in our patient, testicular and para-testicular masses sometimes are misdiagnosed as inguinal hernia or hydrocele[4], especially if the scrotal ultrasonography was not performed in adolescent patients. Conclusion Paratesticular rhabdomyosarcomas are rare neoplasms with aggressive growth patterns. Radical orchiectomy procedure with negative surgical margins is gold standard in the treatment of these tumors. Chemotherapy is recommended for the control of retroperitoneal micrometastases. It is possible to obtain successful results with chemotherapy protocols in these tumors. We think that the scrotal ultrasonography should be done before surgery in all of patients with a painless and painful scrotal mass. Acknowledgment Authors would like to appreciate Dr. Afshin Behbahani for his efforts in management of the patient in intensive care unit. References
© Copyright 2009 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe09055f2.jpg] [pe09055f1.jpg] |
| |||||||||

{kind=link}
{kind=link}