 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 269-276 Effect of Anti-Epileptic Drugs on Serum Level of IgG Subclasses Mahmoud-Reza Ashrafi1,2, MD; Seyed-Ahmad Hosseini2, MD; Mohammad Biglari3, MD; Sarah Abolmaali3, MD; Reza Azizi Malamiri2,4, MD; Hoda Mombeini3, MD; Zahra Pourpak5, MD, PhD; Narges Saladjegheh6; Nima Rezaei2,3, MD, PhD, Shiva Saghafi5, MSc and Asghar Aghamohammadi1,2,3, MD, PhD 1Department
of Pediatrics, Tehran University of Medical Sciences, Tehran, IR Iran Received: Feb 10, 2009; Final Revision: Jun 17, 2009; Accepted: Jul 17, 2009 Code Number: pe10040 Abstract Objective: There
are some controversial studies on effects of anti-epileptic drugs (AEDs)
on serum IgG subclasses; however, the role of these medications is
still unclear. The
aim of this study was evaluation the effects of anti-epileptic drugs
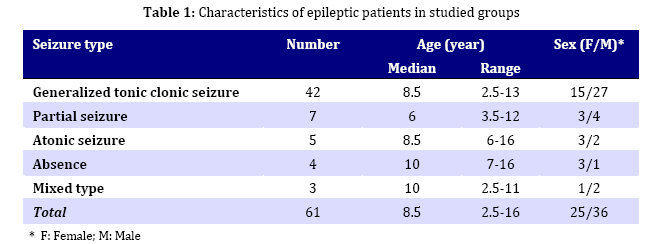
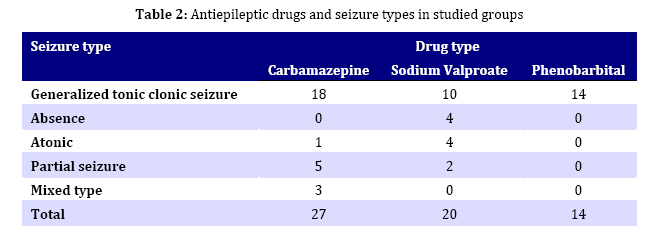
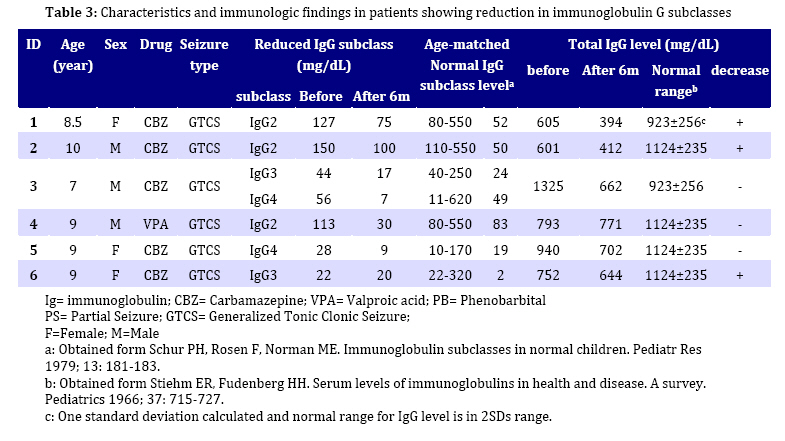
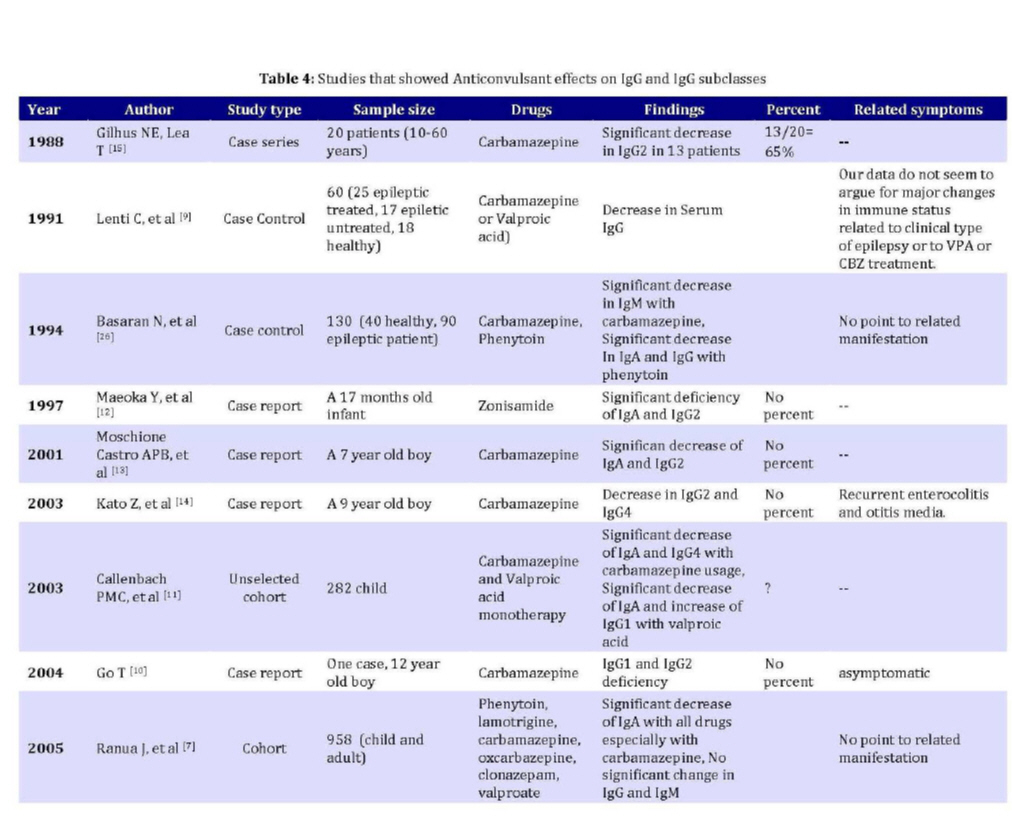
on serum concentration of IgG and its subclasses. Key Words: Antiepileptic drugs; Immunoglobulin G; IgG subclasses; Epilepsy Introduction Epileptic disorders affect 50 million people around the world[1], which is one of the most prevalent diseases of central nervous system (CNS) throughout childhood and adolescence up to 16 years of age[2-4]. There were numerous studies on the presence of immunological alterations in patients with epilepsy and antiepileptic-drug (AED) effects on the immune system. Previous studies showed the possible effects of AEDs on serum immunoglobulin level in epileptic patients[5-8], but there were few studies about AED effects on serum IgG subclasses[9-15]. IgG subclass deficiency induced by AEDs predispose patients to specific infections, whereas asymptomatic patients were also reported[16]. The purpose of this study was to assess the effect of antiepileptic drugs [Carbamazepine (CBZ), Sodium valproate (VPA) or Phenobarbital (PHB)] on serum IgG and its subclass concentrations of 61 newly diagnosed epileptic children and adolescents. Subjects and Methods Sixty one first diagnosed epileptic patients were enrolled in this case series study. Diagnosis of epilepsy was based on history of seizure, physical examination and EEG (Electroencephalography) findings[17,18]. Seizure type classification was done according to the recommendations of the International League Against Epilepsy[19]. Selection of AEDs for each patient was based on pediatric neurologist decision according to seizure type, age, sex, and EEG findings. Inclusion criteria for this study were age older than 2 years, no previous consumption of immunosuppressive or antiepileptic drugs and monotherapy with CBZ, VPA or PHB. The study was conducted at the Outpatient Department of Neurology in Children’s Medical Center affiliated to Tehran University of Medical Sciences (TUMS). This study was reviewed and approved by the Ethics Committee of TUMS. Written informed consent was obtained from children’s parents. IgG subclasses measurement was performed using ELISA method[15]. A reasonable guideline for diagnosis of subclass deficiency is the laboratory analyses performed in Immunology, Asthma and Allergy Research Institute (IAARI) affiliated to TUMS. Venous blood was drawn from each patient just before treatment and after 6 months of AED monotherapy, for measuring IgG and its subclasses. In addition, serum AED concentration was measured at later samples. All serum samples were taken in the morning before AED consumption. The serum samples were stored at -20˚C in different aliquots until analyzed. Serum IgG concentrations were measured by means of nephelometric method, (MininephTM Human IgG Kit, The Binding Site Ltd., Birmingham, UK). The determination of IgG concentration by this method involves a reaction with specific IgG antiserum to form insoluble complexes. By passing light through the formed suspension a portion of the scattered light is detected by a photodiode that is directly proportional to the IgG concentration in the test sample. Serum levels of IgG subclasses (IgG1, IgG2, IgG3 and IgG4) were measured by ELISA kit (Sanquin, Amsterdam, The Netherlands) according to the manufacturer's instruction. Test samples were incubated in microwell strips coated with highly avid monoclonal antibodies, specific for one of the human IgG subclasses; IgG subclass binds to the solid phase, and peroxidase-conjugated anti-human IgG antiserum was added to each well. After incubation with substrate solution and H2O2, the reaction was stopped with acid buffer. The absorbance of green colored reaction product was measured at 405 nm by ELISA reader. A reasonable guideline for diagnosis of subclass deficiency and IgG deficiency is the value less than 2SD (standard deviation) below the mean for age[20,21]. The serum AEDs concentration was measured by High Performance Liquid Chromatography (HPLC) method. The patients were evaluated at monthly intervals for their seizure control, unwanted side effects and manifestations of infectious diseases. Findings Sixty one epileptic patients (36 males and 25 females), aged 2.5-16 years (median: 8.5 years), were studied during an 18-month period. Generalized tonic clonic seizure was the most frequent seizure type identified in 42 patients (68.8%), followed by partial in 7 cases, (11.4%), atonic in 5 cases (8.1%), absence in 4 cases (6.5%), and mixed type seizures in 3 cases (4.9%). Five patients (8.2%) were classified as symptomatic and 56 patients (91.8%) as idiopathic epilepsy. Age, sex and seizure types of patients are shown in table 1. The median period between the first seizure and beginning of treatment was 30 days. Patients were classified into 3 groups according to antiepileptic drugs that were given: 27 patients in CBZ group, 20 patients in VPA group, and 14 patients in PHB group. Characteristics of patients according to drug type are depicted in table 2. The serum concentrations of IgG and its subclasses, obtained before AEDs therapy, were within normal limits, except in one case with decreased IgG level. Significant reduction of at least one IgG subclass was found in 6 patients (9.8%) 6 months after treatment with AEDs that is illustrated in table 3. Reduction of more than 2SD of IgG subclasses as compared with age-matched normal values was considered significant[21]. Among 27 patients receiving CBZ, significant decrease in at least one serum IgG subclass level was found in 5 patients (18.5%). Of these 5 patients, IgG2 was declined in two patients, IgG3 in one patient, IgG4 in one patient, while decrease of both IgG3 and IgG4 was found in another one. Among 20 patients of VPA group, only one patient (5%) showed significant decrease in IgG2 subclass. None of the 14 patients in PHB group showed significant decrease in IgG subclasses. IgG levels declined in three cases of 6 patients with IgG subclass reduction. One of them had reduction in IgG concentration even before reduction in IgG concentration even before treatment, considering the fact that duration between beginning of epilepsy and treatment was 330 days. AED serum concentrations measured in all patients after six months of therapy were in therapeutic levels. Discussion Epileptic disorder is one of the most prevalent diseases of CNS among childhood and adolescence[2-4]. Immune mechanisms may be involved in the pathogenesis of a number of epilepsies such as Rasmussen's encephalitis, Lennox-Gastaut syndrome, Landau-Kleffner syndrome, and temporal lobe epilepsy. Also immunologic abnormalities have been reported in epilepsy, either by direct effect of epilepsy on immune system[22-24] or by effect of antiepileptic-drug (AED) on serum immunoglobulin levels[5-8]. There are several reports concerning the effects of AEDs therapy on humoral and cellular immunity, which are summarized in Table 4. Based on reported studies, frequency of reduction in IgG subclass could be up to 65%, mainly occurring in IgG2 subclass[10,12-15]. Sixty one newly diagnosed epileptic patients were enrolled and their IgG level and its subclasses were measured before and six months after treatment. In our study, the median period between the first seizure and beginning of treatment was 30 days, which is comparable with Dutch study of epilepsy in childhood with a period of 69 days[11]. The IgG subclass of antibodies composed of four different subtypes: IgG1, IgG2, IgG3 and IgG4. IgG1 consists of 66% of IgG, while IgG2, IgG3, and IgG4 consist of 24%, 7%, and 3% of IgG, respectively[25]. The amount of the different IgG subclasses present in the bloodstream varies with age[20]. As shown in Table 3, none of our patients showed IgG subclasses alteration (increment or decrement) at the beginning of treatment, but there was reduction in IgG in one case before beginning of treatment; duration between epilepsy and treatment in this case with decreased IgG was 330 days; it is not clear whether untreated epilepsy could have any effect on immunoglobulin level. This hypothesis needs further investigation. A number of studies decreased IgG was 330 days; it is not clear whether untreated epilepsy could have any effect on immunoglobulin level. This hypothesis needs further investigation. A number of studies on patients and experimental animals indicated that AEDs can induce a decreased humoral immune response[6,15,26-33] while the state of epilepsy or the underlying brain disorder may predispose immunodeficiency even before AEDs treatment[15]. Moreover decrease of IgG2 is not sufficiently pronounced to cause a significant change in the total serum IgG concentration[6], although we observed a decrease of total IgG in one patient. Selective IgG1 subclass deficiency is very rare condition. IgG2 subclass deficiency is the most frequent subclass deficiency in children, while IgG3 subclass deficiency is the most common subclass deficiency in adults. IgG4 deficiency usually occurs in association with IgG2 deficiency. Considering the fact that normal population could have undetectable IgG4, selective IgG4 deficiency is generally not assumed as an immunological defect and not usually of clinical significance[25]. Considering the effects of CBZ on IgGsubclasses, there are some previous studies thatshowed IgG2 decrement after treatment[23-24].Similar to these studies we found two cases withdecrease of IgG2 6 months after therapy.Combined deficiency of IgG1 and IgG2 was alsoreported[10]. We found two cases with decreaseof IgG3 and IgG4; one of them had combineddeficiency of IgG3 and IgG4. Considering theeffects of VPA on IgG subclasses, there is onlyone previous report of increasing IgG1[11].Among 20 patients treated with VPA, only onepatient showed IgG2 deficiency which has notpreviously been reported to our best knowledge.In the Dutch study, a significant decrease of IgG4levels was found in association with CBZ use,while increase in IgG1 level was reported inassociation with using VPA[11]. In another study,an association between CBZ monotherapy and adecrease of IgG2 was described, while IgG4remained unaffected[15]. None of patients treated with PHB showedalteration in IgG subclasses, but further studieswith larger samples for this drug could berecommended. Although the exact mechanisms for IgG subclass deficiencies in the patients usingAEDs are not clear, defect of B cell maturationinduced by AEDs are proposed to be responsiblein this regard[10]. Although an increased risk of susceptibility torecurrent infections, especially respiratory tractinfections, are the most frequentlymanifestations in patients with IgG subclassdeficiencies[34-36], none of our patients withdecrement of IgG subclasses had more frequentrespiratory tract infections than other patientswith normal IgG subclasses, which was similar toprevious study[17]. In respect to the fact that our IgG subclassdeficient patients were asymptomatic, we didnot decide to change or discontinue the drugbecause of its humoral effects. Therefore AEDeffects on IgG subclasses can be asymptomaticwithout clinical significance. The results of this study were limited by thefact of small sample size and short period offollow up. Although in our studeficiencyselective IgG subclass dy, children withwereasymptomatic, we recommend fpractices in epileptic patients undergoingollowingtreatment with AEDs: It is a good practice toassess the serum immunoglobulin levels atstarting the administration of anticonvulsantdrug in an epileptic patient; evaluation of serumimmunoglobulin levels at serial intervals afterbeginning of AEDs could be considered; and it isa good practice to discontinue or change the AEDin an epileptic patient with decreased serumimmunoglobulins. Conclusion
Acknowledgment
Treatment with AEDs is associatedalterations in serum concentrations of withsubclasses and professionals who frequentlyprescribe these drugs should be alert to tIhgGisalteration. Although in our studeficiencyselective IgG subclass dy, children withwereasymptomatic, assessment of serumimmunoglobulin levels could be recommendedat starting the administration of AEDs and inserial intervals afterward in epileptic patients. We are extremely indebted to the authorities ofthe Research Deputy of Tehran University of Medical Sciences for their financial and logistic support (Grant no: 85-04-30-4667). We thank the authorities of the Immunology, Asthma and Allergy Research Institute (IAARI).Our special thanks to L. Foroutan, and M.Shahgaldi. Conflict of Interest: None References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}
{kind=link}
{kind=link}
{kind=link}