 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 277-283 Efficacy of Carvedilol in Patients with Dilated Cardiomyopathy due to Beta-thalassemia major; a Double-blind Randomized Controlled Trial Gholam-Hossein Ajami1, MD; Hamid Amoozgar1, MD; Mohammad Borzouee1, MD; Mehran Karimi2; Farah Piravian2; Afsaneh Ashrafi2; and Zahra Kheirandish2, MD 1Division
of Pediatric Cardiology, Department of Pdiatrics, Shiraz University
of Medical Sciences, IR
Iran Received: May 20, 2009; Final Revision: Dec 18, 2009; Accepted: Feb 20, 2010 Code Number: pe10041 Abstract Objective: Dilated
cardiomyopathy is the end result of chronic iron overload in patients
with beta thalassemia major. The
objective of the present study was to
evaluate the safety and efficacy of Carvedilol in patients with
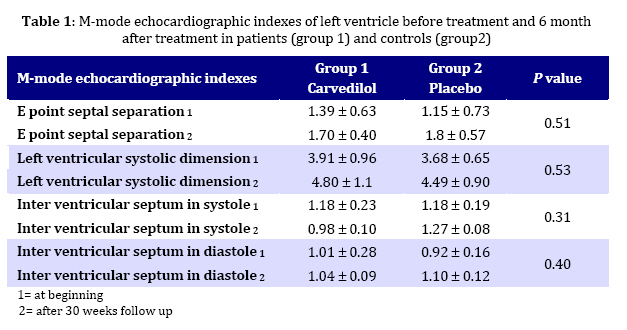
beta thalassemia major and dilated cardiomyopathy. Key Words: Beta thalassemia major; Carvedilol; Heart filure; Dilated cardiomyopathy Introduction Although the use of beta-blocker medications in adults with congestive heart failure (HF) have been explored for over 20 years,[1] their use in children has been very limited[2,3]. Modern management of heart failure has become more than the normalization of cardiac output and the improvement of symptoms. Neuroendocrine stimulation, myocyte remodeling, cellular energetics and connective tissue/myocyte interactions are equally considered when treating children with heart failure[4]. The therapeutic goals include the "normalization" of altered hemodynamics and amelioration of symptoms[5]. To this end point inotropes, vasodilators and diuretics are the drugs used primarily depending on the clinical features of each patient. The use of beta-blockers in the treatment of congestive heart failure in adults has been shown to reduce the risk of hospitalization and death rate in cases with mild-to-moderate heart failure[6,7]. The exact mechanism of action of beta-blocking agents in chronic heart failure is still not entirely clear. The acceptable hypothesis is that the primary mechanism of action of beta-blocking agents in chronic heart failure is to prevent and reverse adrenergically-mediated intrinsic myocardial dysfunction and remodeling[8,9]. First generation beta-blockers (propranolol) are non-selective for beta 1 or beta-2 blockade and have no ancillary properties. Second generation beta blockers (e.g. metoprolol, bisoprolol) are selective for beta-1 or beta-2 blockade, but also have no ancillary properties. Third generation beta-blockers (eg Carvedilol and buncindolol) are either B1 and B2-blockers[10]. Carvedilol, a nonselective third-generation beta-blocker, vasodilator secondary to alpha1-adrenergic blockade with antioxidant activity and apoptosis inhibition has been demonstrated to favorably affect survival in adult patients with severe chronic heart failure[11]. The experience with beta-blockers in children with congestive heart failure is limited and previous studies were not double-blind or randomized with placebo-controlled Group[12-18]. In addition, due to heterogeneity of cardiomyopathy in pediatric patients, the present study was conducted to evaluate the safety and efficacy of Carvedilol in patients with beta-thalassemia major who have a common cause of cardiomyopathy and heart failure. Study was a double blind, randomized and placebo controlled trial. Subjects and Methods Between January 2006 and January 2008, fourteen patients with Beta thalassemia major without diabetes mellitus with ejection fraction less than 55% who were referred to pediatric cardiology clinic were enrolled in this double blind, randomly assigned study. The diagnosis of all patients was proved by complete blood count and hemoglobin electrophoresis. All patients were on regular blood transfusions and received deferoxamine injection irregularly by pump as iron chelating agent, they were all on anti failure therapy with digoxin, captopril and furosemide, two patients in each Group were on Amiodarone for control of arrhythmias as well. The study was approved by committee of ethic of Shiraz University of Medical Sciences and written informed consent was obtained from each patient or parents. Patients were randomly assigned to two Groups by a nurse who was blind to medications which were provided in similar bags, Group 1 received Carvedilol (6.25 mg tablets from PLVA pharma Ltd, Vision Hare, Bedford Road, Peters field, Hampshire GU32 3QB), and Group 2 received placebo (with the similar appearance as Carvedilol made by Shiraz University of Medical Sciences, Pharmacology Department). Patients were visited by the same physician in each visit who was blind to the type of drug received by the patients. Carvedilol was started at a dosage of 3.12 mg bid and for patients who had systolic blood pressures >100 mmHg, and a heart rate >60/min without signs of low cardiac output or respiratory wheeze, the dosage was increased every two weeks to a maximum of 25 mg bid if the patient tolerated the change. Echocardiographic studies were done by Vivid 3 echocardiography machine, probe 3 MHz; Doppler studies and Tissue Doppler indexes were measured by the same probe. Echocardiographic indexes were measured before starting medication, 2 weeks, 4 weeks, 8 weeks, 16 weeks and 30 weeks afterwards. Patients were evaluated clinically on regular basis for evidence of changes in the status of congestive heart failure and complications of medications. Heart rate, blood pressure and central venous pressure (CVP) were measured and patients were evaluated for fatigue, edema, rales, gallop rhythm, diarrhea, rashes, wheezing and New York Heart Association (NYHA) classification. Data were recorded in forms and the results were analyzed, using computer software SPSS 15. Mean values ± one standard deviation in each Group were compared by Mann-Whitney, Wilcoxon and paired sample t-tests, P-value >0.05 was considered statistically significant. Findings The mean age of patients was 16.23±0.71 years in Group 1 and 17.51±3.11 years in Group 2. Mean serum ferritin was 2300 and 2500 ng/mL in Group 1 and Group 2 respectively. Eight patients received Carvedilol and 6 patients received placebo. There was only one male patient in Group 1 and the rest were females. Only one patent in Group1 tolerated increasing dosage of Carvedilol to more than 6.25 mg bid. Other patients received 6.25 mg Carvedilol bid due to a drop in systolic blood pressure to lower than 90 mmHg. Two patients in Group 1 had signs of increasing preload (edema, dyspnea and increasing left ventricular dilatation) so that Furosemide dosage was increased. Clinical evaluation of the patients revealed the following results: Respiratory rate of patients in Group 1 changed from 15.31±5.62/min to 15.44± 1.43/min and in Group 2 from 14.65±1.76/min to 15.22±1.31/min (P=0.8). Pulse rate in Group 1 changed from 82.77±30.84/min to 85.32± 21.56/min and in Group 2 from 90.55± 28.21/min to 82.45±28.25/min (P>0.05). Systolic blood pressure in Group 1 changed from 93.51±10.34 mmHg to 74±22 mmHg and in Group 2 from 105.31±7.25 mmHg to 97±17 mmHg (P=0.07). Diastolic blood pressure in Group 1 changed from 57.35±11.31 mmHg to 60.25±5.31 mmHg and in Group 2 from 55.44±7.51 mmHg to 60±10 mmHg (P=0.1). Jugular venous pressure in Group 1 changed from 10.12±2.57 cm H2O to 11.35±5.61 cm H2O and in Group 2 from 11.51±5.63 cm H2O to 11.35±5.64 cm H2O (P=0.3). Mean NYHA classification in Group 1 changed from 1.75 to 1.55 and in Group 2 there was no change (P=0.1). Echocardiographic data were as follows: M-mode Echocardiography: Ejection fraction in Group 1 changed from 45.55 ± 10.73% to 44.25 ± 9.93% and in Group 2 from 45.56 ± 4.98% to 45.32 ± 8.64 % (P=0.4) figure1. End diastolic dimension in Group 1 changed from 5.52±1.12 cm to 7.22±0.95 cm and in Group 2 from 5.31±0.69 cm to 8.52±1.11 cm (P=0.7). Other data are shown in Table 1. Doppler indexes: E wave velocity of mitral valve in Group 1 changed from 0.69±0.65 m/s to 0.81±0.14 m/s and in Group 2 from 0.85 ± 0.28 m/s to 1.21± 0.10 m/s (P=0.3). A wave velocity of mitral valve in Group 1 changed from 0.62±0.3 m/s to 0.70±0.05 cm/s and in Group 2 from 0.63±0.15 m/s to 0.41±0.09 m/s (P=0.6). E to A wave ratio of mitral valve in Group 1 changed from 1.10±0.37 m/s to 1.81±0.40 m/s and from1.34±0.30 m/s to 2.6±0.23m/s respectively (P=0.04). Pulmonary acceleration time in Group 1 changed from 102.12±25.69 s to 75.02±17 s and in Group 2 from 100.33±4.21 s to 91.23±16.35 s (P=0.4). Other Doppler indexes are shown in Table 2. Tissue Doppler indexes included: Sa wave velocity of lateral mitral annulus in Group 1 changed from 6.75±1.28 cm/s to 5.30±1.41 cm/s and in Group 2 from 6.55±0.01 cm/s to 6.35±0.02 cm/s (P=0.3). Ea wave velocity of lateral mitral annulus in Group 1 changed from 10.62±3.50 cm/s to 9.50±2.25 cm/s and in group 2 from 9.51±0.71 to 7.55±2.12 cm/s (P=0.8). Aa wave velocity of lateral mitral annulus in Group 1 changed from 5.60±2.57 to 4.51±2.12 and in Group 2 from 3.51±0.72 to 3.23± 3.20 cm/s (P=0.6). Other indexes are shown in Table 3. Discussion Restrictive cardiomyopathy is the most common cardiac complication that occurs with iron overload, but other problems including pericarditis, dilated cardiomyopathy, and angina without coronary artery disease have also been described. A strong correlation exists between the cumulative number of blood transfusions and functional cardiac derangements in patients with thalassemia[19]. Echocardiographic assess-ment of patients with beta-thalassemia major who have received concurrent chelation therapy with Desferrioxamine shows no difference compared with controls in the fractional shortening[20]. A pronounced pattern of integrated backscatter of the interventricular septum and posterior wall is an important echocardiographic finding indicating iron deposition. The physical examination reveals surprisingly little even in patients with heavy cardiac iron deposition. Once evidence of cardiac failure appears, however, heart function deteriorates rapidly, often resisting medical intervention. Biventricular failure produces pulmonary congestion, peripheral edema, and hepatic engorgement. Iron deposition in the bundle of His and the Purkinje system impairs signal conduction from the atrial pacemaker to the ventricles. Patients sometimes die suddenly, presumably due to arrhythmias[20]. Unfortunately, due to shortage of deferoxamine in our area in the past and poor compliance of thalassemic patients for using it, many of these patients have developed hemosiderosis and have multiple endocrine organ involvement, like diabetes mellitus. This usually presents before cardiac involvement and because beta blockers mask hypoglycemic symptoms it should be used with caution in poorly controlled diabetic patients. In this study most of the patients who received Carvedilol had a decrease in systolic blood pressure below 100 mmHg. Increasing drug dose to more than 6.25 bid (only one patient tolerated increasing the drug to 12.5 mg bid) inhibited advancing Carvedilol to the full dose (25 mg bid) as recommonded in previous studies on cardiomyopathic patients. During increasing drug doses, we tried to continue other drugs like digoxin and ACE inhibitors and Furosemide at a steady dose but 2 patients in Group 1 had signs of increasing preload (edema, dyspnea and increasing left ventricular dilatation) so the Furosemide dosage was increased. In the management of an exacerbation of HF in patients who have been stable on a beta blocker, regarding the American Heart Association (ACC/AHA) guidelines cardiologists continue the beta blocker and intensify diuretics and other therapies if the exacerbation is primarily due to fluid overload[21,22]. During administration of Carvedilol, after a period of increasing NYHA class there was gradual decreasing. Systolic blood pressure decreased in this group especially during increasing drug to more than 6.25 mg bid. Previous studies have shown that many patients have a substantial period of worsening of HF symptoms, often lasting three to four months after the initiation of beta blocker therapy[22]. The first observation suggesting that beta blockade might be beneficial in HF was made in 1975[25]. Subsequent reports consistently confirmed these findings, demonstrating that over a three- to six-month period of follow-up, beta blockers led to improvements in LVEF (left ventricular ejection fraction) and resting hemodynamics[26-30]. Improvement in contractile function with beta blocker therapy occurs in dysfunctional regions of viable myocardium, but not in regions of extensive scarring[30]. In our study ejection fraction decreased in Carvedilol receiving Group in comparison to control Group during the first 2 months but at the end of 6-mounth follow-up, patients had the same ejection fraction as the control Group. These discrepancies with other studies might be due to difference in type of cardiomyopathy in thalassemic patients in whom there is a restrictive pattern of cardiomyopathy with diastolic dysfunction that gradually produces a dilated cardiomyopathy with systolic dysfunction as end stage result associated with diffuse involvement of myocardium. The present study showed that E to A ratio in Doppler echocardiography increased signify-cantly in control Group, which might be an indicator of worsening diastolic dysfunction and aggravation of restrictive pattern. Although changes in tissue Doppler velocities were not statistically significant, a decrease in Ea velocity in control group was seen which also shows worsening of diastolic function. Limitations of the study: To our knowlage this is the first report on the effect of Carvedilol in adolescents with β-thalassemia major, however the following shortcomings are worthy of mention: First, because of small number of patients included in this study, we consider our results as a preliminary report and more studies with larger population are needed. Secondly, our patients could not receive the full dose of the drug due to decrease in blood pressure that might affect observation of the significant effect of this drug. Conclusion It seems that patients with thalassemia and dilated cardiomyopathy tolerate increasing Carvedilol dosage poorly and develop decrease in systolic blood pressure during advancing the dosage. A period of increasing preload and worsening of HF was seen during first 2 months of starting medication without any improvement of left ventricular function in the first 6 months of therapy with Carvedilol. Carvedilol can be effective in prevention of progression of diastolic dysfunction in patients with beta thalassemia major and dilated cardiomyopathy. Acknowledgment This work was financially supported by the office of the Vice Chancellor for Research of Shiraz University of Medical Sciences. We thank Professor GH Amirhakimi for his thoughtful review of the manuscript, Dr S Mohammadi Samani for preparation of placebos and Mrs. Fatemeh Beladi who kindly followed up the patients. Conflict of Interest: None References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}
{kind=link}
{kind=link}