 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 291-296 Comparing Oral Route Paraffin Oil versus Rectal Route for Disimpaction in Children with Chronic Constipation; a Randomized Control Trial Fatemeh Farahmand1,2, MD; Kambiz Eftekhari2, MD; Vajiheh Modarresi2, MD; Mehri Najafi1,2, MD; Ahmad Khodadad1,2, MD, and Farzaneh Motamed1,2, MD 1Department
of Pediatrics, Faculty of medicine, Tehran University of Medical Sciences,
Tehran, IR Iran Received: Sep 17, 2009; Final Revision: Nov 18, 2009; Accepted: Feb 10, 2010 Code Number: pe10043 Abstract Objective: Functional
constipation is a common and challenging problem in pediatrics. Fecal
disimpaction prior to maintenance therapy is recommended to ensure successful
treatment. The aim of this study was to compare the efficacy and patient’s
compliance of the two methods of paraffin oil administration (oral and
rectal route) with the purpose of disimpaction in treatment of children
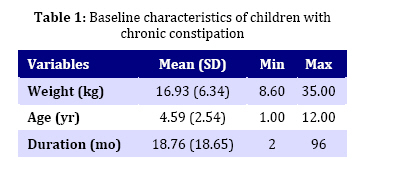
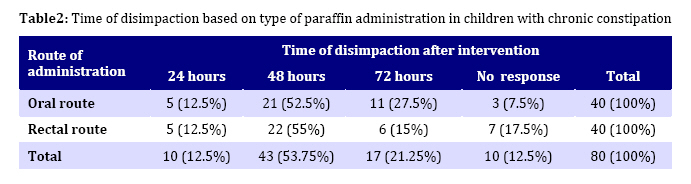
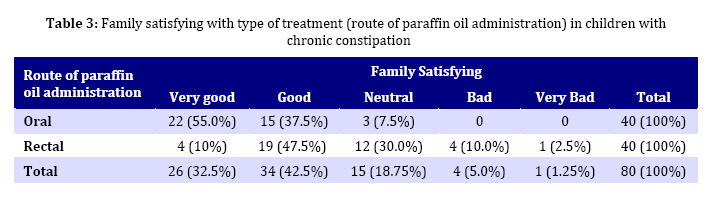
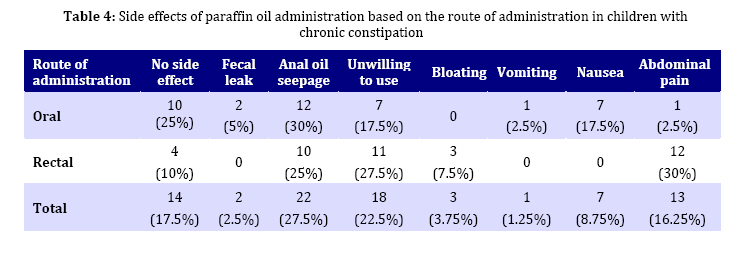
with functional constipation. Key Words: Fecal impaction; Constipation; Chronic constipation; Functional Colonic Diseases; Paraffin oil Introduction Constipation is a common reason of referring a child to a pediatric gastroenterologist. There is no underlying organic disease in 97% of cases[1]. Even though it creates a significant amount of distress and anxiety to the families[2] indeed, it could be the most common cause of acute abdominal pain[3]. Management of chronic constipation in the first step is disimpaction of feces that itself produces more anxiety for the families, especially in an unexperienced family. In the second step, prevention of constipation with increasing fiber intake and using mineral oil (liquid paraffin), lactulose or poly ethylene glycol (PEG) is suggested as a maintenance therapy. Among different methods of medical treatment, fecal disimpaction has priority. There are various methods for disimpaction including, enema and giving various materials orally like bulking agents, osmotic laxatives, lubricating laxatives and stimulating laxatives[4,5]. Successful treatment of fecal impaction with PEG has been reported by Youssef et al[6]. Rectal disimpaction can also be performed with phosphate sodium enema (fleet), saline, or mineral oil enema followed by a phosphate enema[2]; this kind of enema should be used with some caution because of its major complications such as metabolic derangements in serum phosphate, magnesium, sodium, calcium and potassium[7]. In our country, the first line compound usually used for this purpose is paraffin oil[8]. It is also recommended as a first step medication in childhood constipation by North American Society for Pediatric Gastroenterology and Nutrition (NAPSGN)[4]. Mineral (paraffin) oil has been proved as a safe and useful lubricating laxative in the treatment of chronic constipation. It is composed of saturated hydrocarbons obtained from petroleum. It acts by coating and lubricating stools, reducing colonic absorption of fecal water and facilitating the evacuation of the stools. However, lipoid pneumonia as a result of mineral oil aspiration was reported[9]. So, it should not be used in patients with tendency for regurgitation or pulmonary aspiration. In general, it does not interfere with fat soluble vitamins absorption[10]. Although liquid paraffin is the most popular compound as maintenance treatment for constipation, we couldn’t find comparative studies between the two methods of using it for disimpaction in children in the literature. As the parents and child should be involved in the decision regarding the appropriate route, we hypothesize that oral route of disimpaction can be more acceptable, because of less anxiety to the family and suffering child. So, we designed the study to compare the effectiveness and family acceptance of oral method versus rectal method of using paraffin oil in disimpaction of childhood constipation. Subjects and Methods A prospective randomized clinical trial study was performed on 80 children with diagnosis of functional constipation referred to pediatric gastroenterology clinic of Children's Medical Center. Physical examination showed fecal impaction. According to Rome III criteria, functional constipation was defined as having two out of the following symptoms for at least two months: ≤2 defecations per week, ≥1 episode per week of incontinence after the acquisition of toileting skills, history of excessive stool retention or history of painful or hard bowel movements, presence of large fecal mass in the rectum, history of large diameter stools that may obstruct the toilet for children <4 years[11,12]. The study had two parallel groups, single blind, and randomized, prospective comparative design and was performed in the academic Children's Medical Center in Iran. The study was approved by the research ethics board of the Children's Medical Center and written informed consent was obtained from the parents. Baseline characteristics including sex, age, weight, duration of the problem, and finding of rectal examination was recorded for every patient in interview with his/her parents and after physical examination. Then patients were assigned into two groups by simple randomized sampling method. Group I (23 males and 17 females) received 3ml/kg/day liquid paraffin oil per oral route in two divided doses; and Group II (26 males and 14 females) received the same dose of paraffin rectally. Both groups were asked to increase daily fiber intake and try to defecate after each meal for 15 minutes (three times a day). During treatment parents were asked to record clinical efficacy and tolerability as well as side effects of the medication in a dairy. After 3 days of intervention, efficacy, time of response, tolerability, patients' and parents' compliance were assessed using scored questionnaire and all patients were examined again for detecting the fecal impaction by a second examiner. Treatment was interpreted successful if rectal examination revealed no fecal impaction; and remaining fecal impaction was defined as unsuccessful treatment. Family satisfying was evaluated based on recorded dairy that was filled out by parents and classified into very good, good, neutral, bad and very bad scores. Collected data was analyzed statistically by SPSS software 11.5, and tested by Student's t test or non-parametric Mann-Whitney U tests according to the distribution of values. P-value less than 0.05 was considered significant. Findings Within one year, 80 children (aged 1-12 years) with chronic functional constipation and fecal impaction were enrolled in the study; their characteristics are shown in Table 1. The patients were followed up by gastroenterologist. Successful treatment after intervention was found in 70 cases from 80 patients (87.5%) without considering the type of treatment. As shown in Table 2, desired response in Group I was seen in 37 of 40(92.5%) patients and response to the treatment for the Group II was seen in 33 out of 40 (82.5%) patients. Comparing the results of the two Groups, oral paraffin oil yielded better response results, but it was not statistically significant (P=0.1). As shown in Table 2, the majority of patients, 65% in group one and 67.5% in group 2, responded to the treatment after 48 hours. The overall success rate after 48 hours treatment is shown in Table 3. Significantly higher numbers (22 out of 40 vs 4 out of 40) of families were very satisfied with oral route of the treatment (P=0.001). 87.5% of the parents in Group I and 57.5% in Group II found the method of paraffin oil administration very good or good. While 12.5% of parents were unsatisfied with rectal route of paraffin oil administration. No parents recorded bad or very bad scores for type of administration in Group I. Side effects are shown in Table 4. The most common side effect was oil seepage in both groups (27.5%). Nausea and unwilling to take the drug were more common (17.5%) side effects in Group I while abdominal pain was the most common (30%) side effect in Group I, 27.5% of patients in Group II found the method of drug administration, unpleasant. Discussion Despite its common and benign nature, constipation creates a significant amount of distress and anxiety for families. 30-50% of children with functional constipation will continue to have prolonged symptoms despite initial intensive medical management. The treatment is long-lasting and relapses are common. Since the most common reason of treatment failure is non-compliant family, working closely with the families, educating the child and parents are necessary for successful treatment[2]. In this study we found that there is no significant difference in efficacy of the treatment between the two methods of oral and rectal routes of paraffin oil administration for disimpaction. Desirable successful treatment in both Groups was 92.5% and 82.5%. We showed that paraffin oil can be a useful agent for this purpose. In one previous study that compared response rate to lactulose and paraffin oil in 247 patients, the author concluded that paraffin oil is more effective than lactulose in maintenance therapy in functional constipation of children[8]. Urganci et al also compared efficacy, safety and optimal dose of two laxatives, liquid paraffin and lactulose, in two parallel groups (each 20 cases) of children with chronic functional constipation and concluded that patients treated with liquid paraffin responded more rapidly than patients receiving lactulose and showed fewer side-effects[13]. Comparing the two methods of administratiing paraffin oil 3 ml/kg/day by oral route versus rectal route we found a better family compliance when administered orally. In general 87.5% of parents in Group I and 57.5% in Group II were satisfied with the route of drug administration. 12.5% of parents in group II recorded bad and very bad scores for type of administration while no parents in group I complained about type of drug administration. Reviewing Baker et al study that compared two methods of disimpaction, revealed that disimpaction with oral medication is effective if high doses of mineral oil, poly ethylene glycol electrolyte solution, or both are used. They also recommended designing a controlled trial study to compare oral route and rectal route of disimpaction[14]. Although slower response to oral route of disimpaction in comparison with enema was previously reported[15], our study proved that oral route can result in disimpaction within 48 h after taking mineral oil as rapidly as rectal route. In our study, the side effects of oral route were fewer and less important than those of rectal route, which is in agreement with results of other studies[10,13]. However, our study showed that abdominal pain as an unusual side effect in Group 1 in comparison to Group 2 (2.5% vs 30%); more common side effects were oil seepage and nausea in Group 1 (30% vs 17.5%) and abdominal pain and oil seepage in group 2 (30% vs 25%). 10% of patients in Group I and 2.5% of cases in Group II showed no side effects. Dosage of paraffin oil in this study was 3 ml/kg/day that was slightly higher than the dose given in other studies (1.72±0.13 ml/kg/ day)[2,10,13]. The high dose of paraffin that we used in our study, showed no significant additional side effects in comparing to other studies. Some limitations should be taken into account. First, because of lack of quantified parameters, we used clinical symptoms and individual judgment for assessment of family satisfying that led to some unavoidable biases. Second, the relatively low number of patients in this study, although comparable to those in other studies, may have underpowered the significance of differences between patient groups. Conclusion The results showed that administering paraffin oil per oral route was more acceptable with fewer and less important side effects than using it per rectal route; most of the cases preferred the oral route. As we know, the main part of the treatment in children with constipation are; children's compliance and parent's participation. It seems that using paraffin oil per oral route for disimpaction in patients aged 1 year - 15 years who are suffering from chronic functional constipation could be a preferred option, considering the fact that it should not be used for the patients who are at risk for aspiration and avoiding to feed paraffin oil with force. Since mineral oil is the most common compound that is used for treatment of functional constipation in our country, we recommend designing more clinical trials. Acknowledgment The authors thank Research Board of the Children's Medical Center for their cooperation, Dr Nima Rezaee for editorial assistance, Dr Zahra Khazaee for statistical analysis and Maral Sayyad for assistance with the tables. Conflict of Interest: None References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}
{kind=link}
{kind=link}
{kind=link}