 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 308-312 Frequency of Sensory Neural Hearing Loss in Major Beta-Thalassemias in Southern Iran Abolhassan Faramarzi1, MD; Mehran Karimi2, MD; Seyed-Taghi Heydari3, PhD; Mahmoud Shishegar1, MD, and Masoud Kaviani1, MD 1Department
of Otolaryngology Head & Neck Surgery, Shiraz University
of Medical Sciences, Shiraz, IR Iran Received: Jul 01, 2009; Final Revision: Dec 08, 2009; Accepted: Jan 18, 2010 Code Number: pe10046 Abstract Objective: The
thalassemias are among the most common genetic disorders worldwide, occurring
more frequently in the Mediterranean region. The aim of this study was
to determined frequency of sensory-neural hearing loss in major ß-
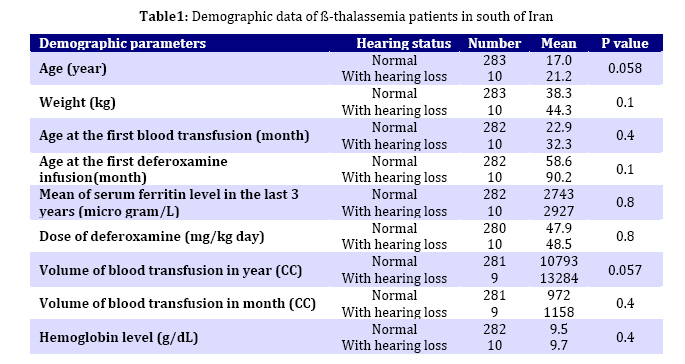
thalassemias transfusion dependent patients in south of Iran. Key Words: Beta-Thalassemia; Sensorineural Hearing Loss; Blood Transfusion; Deferoxamine; Ferritin Introduction The thalassemias are among the most common genetic disorders worldwide, occurring more frequently in the Mediterranean region, the Indian subcontinent, Southeast Asia, and West Africa. Some authors found that about 20%-29% of cases suffering from sensory- neural hearing loss (SNHL).They proposed deferoxamine (DFO) gives rise to SNHL[1,2]. However others have challenged this idea and believed that the incidence of SNHL in β-thalassemias is not higher than general population[3,4]. Injection of 600 mg DFO/kg per day for 30 days in guinea pigs, increased auditory thresholds and loss of inner ear hair cells[5]. In contrast, no effect on auditory function had been found in studies of chinchilla and mice[6,7]. In a research by Ryals et al., in the experimental quail, DFO was injected daily for 30 days at either 750 mg/kg or 300 mg/kg body weight[8]. These dosages were above the limits considered potentially ototoxic in humans. Then the morphology of the supporting cells and hair cells was studied. At the higher dose of deferoxamine, morphological changes were intensified and began to extend to hair cells. They perceived that DFO clearly has the potential to cause damage to the avian inner ear. Ryals et al's study suggests that high doses and prolonged administration of the drug are required for this toxicity to be observable[8]. Because of these controversies and large variability in incidence of SNHL in these patient in the English literatures and because Fars province is a place with high prevalence of the thalassemias in Iran it is worth studying the prevalence of SNHL in relatively large and adequate population of these patients, in order to provide hearing monitoring protocols for this population in the era of managed care. Subjects and Methods We undertook cross sectional study on 308 cases of major beta-thalassemia patients referring to Thalassemia Center of Shiraz University of Medical Sciences between 2006-2007 years. The study was approved by Shiraz Medical Sciences ethics committee and written consent was taken before starting the study. Exclusion criteria were: cases with past-history of ear operation (such as tympanomastoidectomy, myringotomy and ventilation tube); individuals exposed to ototoxic medication except DFO; cases with preexistence hearing loss and abnormal physical exams (such as chronic otitis media; otitis media with effusion, myringosclerosis). The diagnosis of ß- thalassemia major was based on clinical history, complete blood count and hemoglobine electrophoresis. All enrolled patients underwent an otolaryngological visit, microscopic otoscopy. Clinical data such as serum ferritin level, DFO dose, mean daily doses of DFO (mg/kg), mean of serum ferritin level in last 3 years, volume of transfusion of pack cell, mean hemoglobin and hearing status were recorded in a specially formatted questionnaire. Variables that used for evaluation of hearing status were pure tone air and bone conduction thresholds of 250–8000 Hz, speech discrimination threshold (SDS) and speech reception threshold (SRT). Normal hearing was defined as being between 0 and 20 decibels (dB), and ototxicity as a hearing loss of 20 dB or more at two or more adjacent frequencies[9]. Statistical Analysis was performed using statistical analysis software SPSS software version 11.5. The descriptive variables such as mean, median, standard deviations were used. Chi Square was performed for compare of information about a group of patients with hearing loss and without hearing loss. The P value less than 0.05 was considered significant. Findings From total 308 cases of major beta-thalassemia, 15 cases were excluded from the study due to abnormal otologic history or physical examination. Regarding otologic history, there were 4 cases with history of ear operation (two cases with tympanomastoidectomy and one case with myringotomy and ventilation tube) and one case had positive history of hearing loss since 6 months old. We detected 10 cases with abnormal physical exams: 7 case had otitis media with effusion, and 3 case had myringosclerosis Finally 283 (96.5%) had normal hearing and 10 (3.5%) abnormal hearing. Of these patients, 5 had bilateral symmetric hearing loss and 5 unilateral. There was no statically significant difference between two groups regarding mean age, weight, age at the first blood transfusion, age at the first DFO infusion (Table 1). Prevalence of right ear sensory-neural hearing loss in frequencies of 250, 500, 1000 and 2000 Hz was zero, in 3000 Hz, 0.3%, in 4000 Hz, 1%, and in 8000 Hz, 2.6%. In left ear in frequencies of 250, 500, 1000 Hz was zero, in 2000, 3000, 4000 Hz, 0.3% and in 8000 Hz was 2.3%. There were 7 patients with sensory-neural hearing loss hearing loss in only one frequency and 3 patients (1% of patients) in 2 or more consecutive frequency. Discussion Not much was known about the impact of the major β-thalassemia disease and the toxicity of DFO therapy on hearing organ in southern Iran. We found an incidence of only 3.5% SNHL in a large population of patients. In fact conflicting reports and great discrepancy between the incidences of hearing impairment has a long and rich history. It has appeared in the literature during the past 30 years. The first experience of de Virgiliis group in 1975 when they reported high-tone sensorineural hearing loss in 14 of 20 patients with beta-thalassaemia major[10], and later in 1979 when the same group reported moderate unilateral or bilateral high-tone sensorineural deafness in 43 of 75 patients, however, all patients were receiving chelation therapy with DFO, but de Virgiliis et al did not consider this to be causative[11]. Several authors have studied the ototoxicity of DFO, Some studies have reported frequencies of SNHL between 7.4% and 33%[2,12]. Despite small sample size in most of the studies, no statistically significant differences were found between the affected and unaffected groups with respect to age, ferritin levels or lengths of time that they had received and dose of DFO, peak DFO dose and iron overload[2,4,12-14]. The therapeutic index suggested by Porter et al[15] also was not helpful in predicting risk for ototoxicity[2]. The prevalence of hearing loss in thalassaemia patients in other studies were 25% in Olivieri et al (n=89), 33% in Barratt et al. (n=27)[14], 24% in Porter et al. (n= 37)[15], 15.5% in Argiolu et al (n=308)[13], 27% in Kontzolglulou et al (n=88)[14], 29% in Styles et al (n=28)[2] and 3.4% in our study. In a recent study by Shamsian et al. they found the incidence of 7.4% SNHL in 67 patients suffered from major β-thalassemia who treated with deferoxamine. They defined hearing loss as a hearing threshold more than 15 dB. Although they did not report what frequencies involved specifically, the researchers detected there was no association between serum ferritin level or DFO dosage and hearing loss[16]. Although there is discrepancy in the rates between our study and foregoing reports, the difference may be as a result of our definition for hearing loss, ototoxicity, and exclusion criteria. We reviewed the audiograms of Barratt et al study[12]; three of those patients, had a history of recurrent acute ear infections. In three patients whose hearing loss was only above 6 kHz, bone conduction could not be assessed by the authors. We also reviewed the findings of Porter et al[15] Survey, from all 9 cases, in 5 patients hearing loss was only in one frequency above 6 kHz. Actually in Styles and Vichinsky's[2] study we see that of nine patients with abnormal audiograms in 5 of them one frequency was abnormal. In a research by Karimi et al, 128 patients receiving subcutaneous DFO in doses from 21 to 39 mg/kg/day were studied in 2002. Patients had received their total weekly dose of DFO according to two different methods. The first group had received it on an every other day basis and the second group had received it on 6 days a week. Of the patients in the first group 44.7% had hearing loss in the right ear and 41.8% in the left ear only at 8000 Hz frequency, compared to the second group, 27.8 and 23%, respectively. A significant correlation was found between the dose of drug given at each episode of DFO therapy and hearing loss at the frequency of 8,000 Hz. They concluded that DFO ototoxicity is determined not only by the total amount of the drug given, but also by its maximal plasma concentration[17]. However they reported higher frequency of SNHL than other authors, they considered that hearing loss was significant only at one (8000 Hz) frequency. A retrospective controlled study by Masala et[18] al showed a 12% rate of SNHL in patients with thalassemia treated with DFO. The control group of normal patients showed a 10% rate of SNHL. They found no significant difference between thalassemic patients and controls, and concluded that there were inadequate data for DFO otoxicity. Similar findings were reported by Cohen et al who found that 49 out of 52 patients treated with DFO, had no auditory or visual abnormalities[19]. The lack of ototoxic side effects at lower doses can be considered in good harmony with clinical reports of the low incidence of toxic side effects of DFO[5, 20-23]. In a recent national health survey by Agrawal et al, on the prevalence of hearing loss among US adults, they found in the youngest age group (20-29 years), 8.5% showed high -frequency hearing loss, and the prevalence seems to be growing among this age group[24]. Other authors have agreed with this opinion that the DFO dose generally used (<50 mg kg/ day) is not ototoxic. They report a frequency of hearing loss similar to that in the normal population. Ambrosetti et al[4] in a review of 38 adult patients with thalassemia major support this view since in their patients SNHL was related to neither therapeutic index, nor serum ferritin levels. Furthermore, the percentage of patients with SNHL is similar to that in the normal population of the same age (15–35%). Ambrosetti et al. data suggest that no difference exists between thalassemic patients and non-thalassemic population, and it is adequate to conclude that DFO is not ototoxic[4]. Conclusion We herein report the lowest incidence of hearing impairment in a large population of patients suffered from major thalassemia who received deferoxamine. We did not find difference between patients with and without SNHL regarding mean age, weight, age at the first blood transfusion and age at the first DFO infusion. We found that desferrioxamine is not ototoxic at a low dose, as a whole there has been much critical misrepresentation and conflicting data about desferrioxamine ototoxicity in literature. This study presents new statistically valid information to physicians to help them a proper decision making regarding otologic problem in such cases. And the authors emphasize that physicians must attempt to clarify the other causes of hearing loss in patients suffered from thalassemia. Therefore hearing monitoring protocol must be structured according to the particular characteristics of each individual patient, such as age, capability to respond to the audiologic tests, and clinical status. Acknowledgment This work was supported by a grant from Voice Chancellor for Research of Shiraz University of Medical Sciences and Dr Rooshanzamir for data collation. Conflict of Interest: None References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}