 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 323-329 The Value of Serum Uric Acid as a Mortality Prediction in Critically Ill Children Nakysa Hooman1, MD; Mitra Mehrazma2, MD; Shahrbanoo Nakhaii1, MD; Hasan Otukesh1, MD; Maziar Moradi-Lakeh3, MD; Neda Dianati-Maleki4, and Arash Ehteshami-Afshar4 1Department
of Pediatrics, Ali- Asghar Children Hospital, Iran University of Medical
Sciences, Tehran, IR Iran Received: May 15, 2009; Final Revision: Feb 15, 2010; Accepted: Mar 30, 2010 Code Number: pe10048 Abstract Objective: The
role of initial serum uric acid on admission in critically ill patients
is controversial; we presumed that uric acid level can predict the mortality
of the admitted patients to intensive care unit as
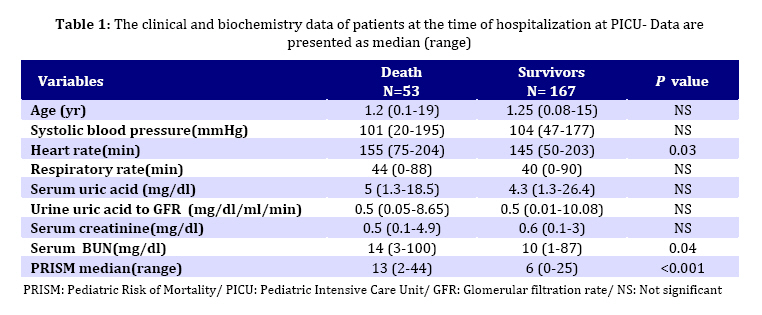
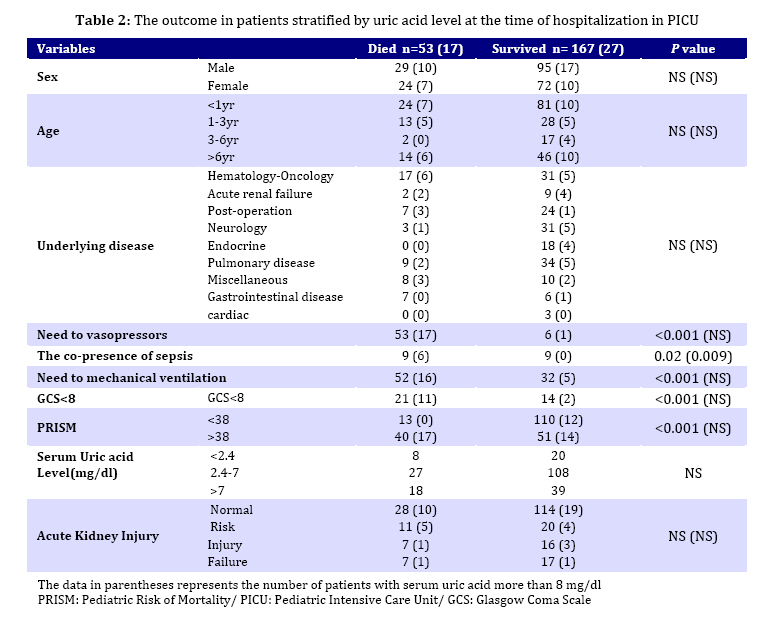
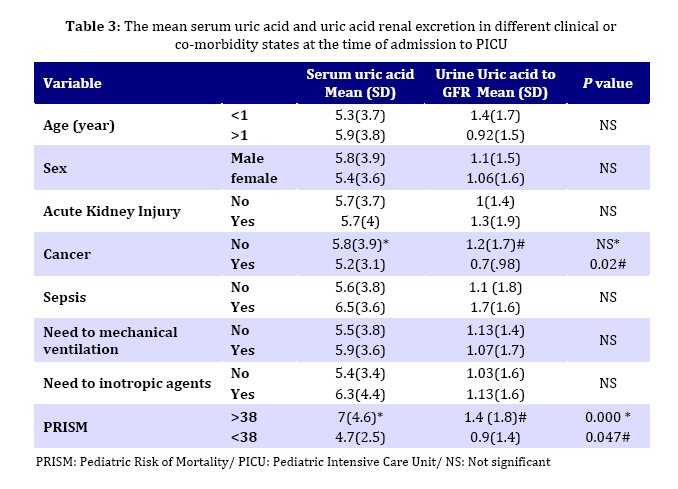
a simple test. Key Words: Uric Acid; Mortality; Intensive care; Pediatrics; Sepsis; Hyperuricemia Introduction Uric acid is an end product of purine base metabolism and an antioxidant agent. Serum uric acid concentration is influenced by several factors such as overproduction, decreased glomerular filtration or renal hypoperfusion, enhanced tubular reabsorption or diminished elimination. It was shown that serum uric acid level was changed in more severe sepsis patients[1-4]. The role of uric acid as an independent causative or potential risk factor of mortality is controversial in patients with kidney disease, hypertension, obesity, cardiovascular events, diabetes mellitus, ischemic stroke and cancer disease[5-14]. There has been found a correlation between serum uric acid level and inflammatory markers on population based cohort studies[15,16]. There are a few surveys on the role of acute increment of uric acid in critically ill cases[17-20] suggesting that marked hyperuricameia in patients with more severe diseases was associated with poor to fatal outcome. Hyperuricemia is associated with acute kidney injury and management with urate oxidase in infants improves the renal function by increasing urine output and declining serum creatinine[21]. Wasserman et al evaluated the effect of serum uric acid on admission on short outcome of adult patients with different co-morbidities and found the serum uric acid as an independent factor of mortality in this population[22]. Several scoring systems have been designed to predict the severity and mortality of children admitted to intensive care units. These scoring systems contain many items that should be checked in various hours after admission which sometimes are very time consuming. We presumed that uric acid level at the early hours of admission can predict the mortality of the admitted patients as a simple single test. This study was conducted to evaluate the validity of serum uric acid in prediction of mortality in pediatric patients in intensive care unit. Subjects and Methods A prospective cohort study was conducted during January 2006 to December 2007 in pediatric intensive care unit (PICU) of Ali-Asghar Children's Hospital in Tehran. This unit contains 6 active PICU beds. Two-hundred twenty consecutively admitted 1-19 year old children were enrolled in the survey regardless of the underlying disease. Inclusion criteria consisted of: first admission of the patient in intensive care unit, staying at least 24 hours at PICU, and taking sample tests before starting any medications. Patients with chronic renal failure, those who stayed less than 24 hours in PICU, those with subsequent PICU admission in the same hospitalization, and those who were discharged from the hospital and then re-admitted to the PICU during the observation period, were excluded. Consent was taken from parents before taking any blood sample. The study was approved by ethical committee of Iran University of Medical Sciences and followed by the institution’s Review Board for Human Subjects guidelines. Clinical and demographic data were recorded by two physicians. Blood sample was drawn and urine sample collected for measuring urine uric acid (mg/dl) to glomerular filtration rate (ml/min) ratio (UUA/GFR) at the time of ICU admission. Colorimetry and uricase method (uric acid TOOS kit, Pars Azmoon Co, Iran) were used to measure uric acid level with Selectra E device. Pediatric Risk of Mortality (PRISM) scores were estimated in 24 hours of PICU hospitalization[23]. Acute kidney Injury was defined according to modified pediatric-RIFLE (risk, injury, failure, loss, and end-stage renal disease) classification[24] based on the estimated clearance of creatinine (eClCr) or urine output at the time of admission. This realizes: Risk (decrease in eClCr equal or more than 25%, or urine output <0.5ml/kg/h for 6 hours), Injury (decrease in eClCr >= 50% or urine output <0.5ml/kg/h for 12 hours), and Failure (decrease in eClCr >=75%, or urine output <0.3 ml/kg/h or anuria for more than 12 hours). Death or transfer from PICU was considered as final outcome. Analyses were performed using SPSS 16.0 for Windows. Independent Student t–test was used to compare the means and Mann-Whitney to compare medians. Linear regression was utilized to find any correlation between outcome and serum uric acid, confounding and underlying variables. The receiver operating characteristic (ROC) curve area evaluated the validity of mortality prediction by serum uric acid level, and risk ratio was calculated by Chi square 2×2 tables. P value less than 0.05 was considered significant. Findings During observation period, 37 out of 257 cases who were consequently admitted to PICU did not imply inclusion criteria (12 cases had chronic renal failure and 25 were re-admitted); so they were excluded from the study. Among them only 3 cases died. 220 children (96 girls, 124 boys) had a mean age of 3.5 years (±4.2 SD). All of the 40 oncologic patients were under chemotherapy. The frequency of death was 24% (53 out of 220) in patients who entered into the study. The demographic and clinical data of patients are shown in Table 1. The mean heart rate, serum blood urea nitrogen, and PRISM score were significantly higher in not-survived cases. Table 2 shows the outcome in patients stratified by serum uric acid level. The mortality was higher in the cases that needed vasopressor, mechanical ventilation, with sepsis, low Glascow coma scale (GCS), or high PRISM score. By adding high uric acid as a cofactor, only patients with sepsis had significantly higher mortality. As shown in Table 3 the mean serum uric acid and renal uric acid excretion were significantly higher in patients with higher PRISM. By backward linear regression analysis serum uric acid showed significant statistical correlation with PRISM score higher than 38 (r=0.31, P<0.001). There was no correlation with sex, age, GCS<9, need to vasopressor or mechanical ventilation, sepsis, diabetic ketoacidosis, acute kidney injury, or cancer disease (P>0.05). Cut point 8 mg/dl was found for serum uric acid level by using receiver operating characteristic curve (ROC) (area under the curve 0.56 and CI95%: 0.46-0.65) that had low sensitivity (32.1 CI95%: 19.9-46.3) and relatively higher specificity (83.8 CI95%: 77.4-89.1) for prediction of mortality. Generally patients with serum uric acid level of more than 8 mg/dl showed with 1.88 (CI95%: 1.17-3) relatively higher risk of death (P=0.02). Using stepwise method in linear regression analysis showed that the need to mechanical ventilation (P=0.001) and vasopressor had statistically significant correlation with the death outcome (P=0.001). On the other hand, there was no correlation between outcome and serum uric acid level of more than 8 mg/dl, GCS <9, PRISM >38, the presence of sepsis, gender, age, acute kidney injury, or underlying disease (P>0.05). The patients with serum uric acid more than 8 mg/dl and needing vasopressor had with 1.04 relative risk (CI95%: 0.9-1.2) a higher risk of death (P>0.05). Likewise, in those under mechanical ventilation with the same uric acid Discussion This study showed that patients with higher uric acid level had higher risk of mortality regardless of the underlying disease. Children with uric acid level of more than 8 mg/dl had two fold risk of death. Mechanical ventilation and vasopressor need were the most independent variables correlated with poor outcome. Children with sepsis who had higher serum uric acid level showed also poor outcome. Few data are available about the prognostic value of serum uric acid in pediatric intensive care unit[17,25]. Chen et al observed that ill children with hyperuricemia had higher mortality rate (50% vs 10%) compared to those who had normal uric acid level. However those patients had more hemodynamically unstable condition than survived patients[17]. Woolliscroft et al compared serum uric acid and uric acid excretion in patients with acute cardiovascular disease and showed that patients with higher and rising uric acid level and lower uric acid excretion had higher mortality rate. These cases had lower blood pressure and worse circulation as well[18]. Besides that infants who underwent cardiac surgery and had very high postoperative serum uric acid level either developed anuric acute renal failure[25] or died[26]. Acute change of serum uric acid is a reflection of overproduction, hemodynamic instability, and change in tubular handling. In our study groups, however, there was no statistically significant correlation between serum uric acid level and blood pressure, heart rate, or decrease in urine output. It was shown that elevation of serum uric acid was correlated directly with increased pulmonary vascular resistance and conversely with decreased cardiac index, as a marker of hemodynamic state, in adult patients with primary pulmonary hypertension or Eisenmenger syndrome who had higher mortality[27,28]. Lazzeri et al found that higher uric acid level had an independent prognostic value of in-hospital mortality among patients with myocardial infarction who had elevated ST segments[19]. In our study patients with hyperuricemia had higher blood urea nitrogen, this means that these cases had decreased glomerular filtration or enhanced tubular reabsorption. Several mechanisms have been proposed for uric acid to potentiate acute renal failure such as renal vasconstriction through impaired endothelial nitric oxide production, inhibit endothelial proliferation and apoptosis induction, inflamatory cells recruitment and releasing of oxidant and inflamatory mediators, and impaired renal autoregulation by developing preglomerular arteriopathy[29]. There was no statistical correlation between rising serum uric acid and acute kidney injury in our study group. We observed that children with sepsis and hyperuricemia had higher risk of mortality; however, the number of patients with sepsis was small. Even though higher total antioxidant status was seen in ill patients[2], uric acid was the predominant measured antioxidant representing renal failure[3] in these cases. A large cohort study showed that adult patients with cancer disease who had serum uric acid level of higher than 6.7 mg/dl had higher risk of mortality and on subgroup analysis detected that hazard ratio was higher for those younger than 65 years. Therefore, they doubt about the role of antioxidant of uric acid in these cases[12]. Molinos et al reported that higher uric acid level on admission to PICU was correlated with mortality and morbidity due to meningococcemia. They found a weak but statistically significant correlation between initial serum uric acid and PRISM during the first day of hospitalization[30]. We observed that those with higher risk of mortality estimated with PRMS had higher mean serum uric acid but using linear regression ananlysis did not confirm any statistical correlation. The need to mechanical ventilation was a major risk factor of death in our study group. When they were stratified by uric acid level, it was detected that 76% of cases who were under mechanical ventilation and had high level of serum uric acid did not survive. This figure was 4.3% in those who were not under mechanical ventilation but had high serum uric acid level. This might be related to underestimation of the necessary fluid leading to renal underperfusion and increased reabsorption of uric acid from the proximal tubules as a physiologic reponse. Despite serum acid level, more than 90% of hypertensive patients who needed inotropic agents died but all patients with normal blood pressure survived. This shows that serum uric acid had no additive adverse effect in this population but only increased the risk of mortality in association with sepsis. A combination of multifactorial events such as hypovolemia, sepsis, drug nephrotoxicity, hemodynamic instability, severity of the underlying disease and its complications, and nosocomial infections may influence outcome of the patients admitted to PICU; therfore, the course of what happens during the following days might be as important as the initial condition of the patients. Although our findings were not convincingly distinctive, but we suggest that the consequent measurment of serum uric acid with recording all changes in the course of management might prognosticate better than a single measurment at the first day of admission that was one of the limitations of the present study. In addition, the nonhemogenous samples could induce a bias in the study. Conclusion Uric acid level during the first day of intensive critical care admission is not an independent risk of mortality in PICU. The effect of mechanical ventilation and resistant shock regardless seum uric acid level were the major factors that determined the outcome. Although the presence of sepsis and high level of uric acid were associated with poor outcome. Acknowledgment The study was supported by Iran University of Medical Sciences grant number 657 dated 2005. Conflict of Interest: None References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}
{kind=link}
{kind=link}