 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 330-334 Breastfeeding and Helicobacter Pylori Infection in Children with Digestive Symptoms Maryam Monajemzadeh1, MD; Fatemeh Farahmand2,3, MD; Fatemeh Vakilian4, MD; Fatemeh Mahjoub1, MD; Milad Alam5, BS, and Nasim Kashef6, PhD 1Department
of Pathology, Tehran University of Medical Sciences, Tehran, IR Iran Received: Jul 22, 2009; Final Revision: Dec 27, 2009; Accepted: Apr 30, 2010 Code Number: pe10049 Abstract Objective: This
study aims to evaluate the role of breastfeeding in the acquisition
of Helicobacter pylori (H. pylori) infection in Iran and to
compare the histopathologic changes occurring in children feeding on
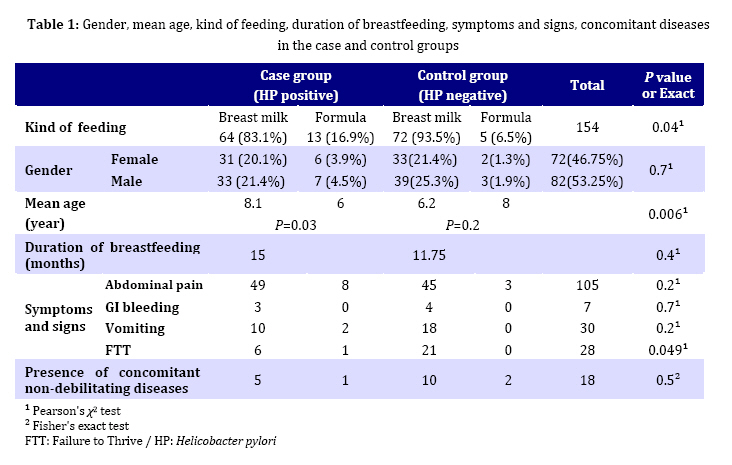
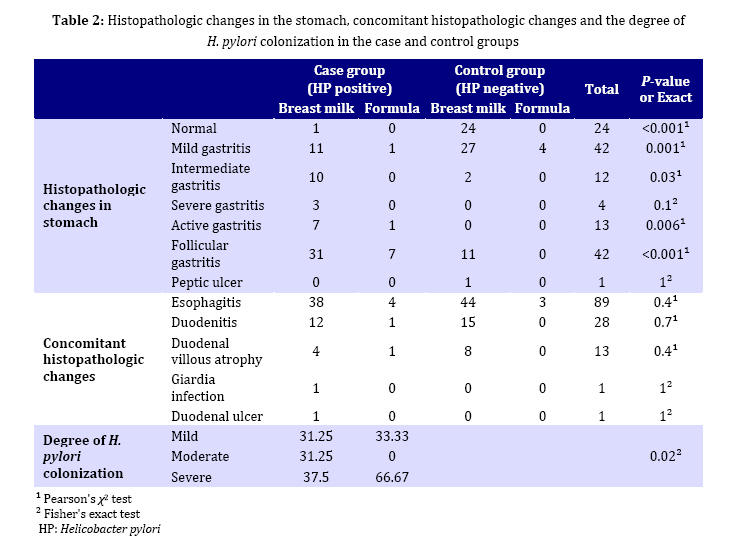
breast milk with those in infants feeding on formula. Key Words: Breastfeeding; Gastritis; Helicopter pylori; Formula Introduction Helicobacter pylori, a gram negative bacillus, is recognized as the main etiological agent of several gastroduodenal diseases including peptic ulcer and gastric malignancies. Breastfeeding, while providing protection against many infective agents, can facilitate the acquisition of H. pylori infection. This infection occurs as a result of the close contact between breastfeeding child and the infected mother. Some studies have shown breastfeeding’s protective effect against the acquisition of H. pylori infection[1-4]. Contrastingly, other studies have reported that breastfeeding does not have a protective effect against the acquisition of H. pylori infection[5-7]. Furthermore, these studies have suggested that breastfeeding can even increase the rate of infection, especially in children breastfed for longer than 6 months[8]. Such different results might stem from the differences in the social and cultural practices of breastfeeding. Despite this plausible explanation, no studies have yet explored the role of breastfeeding in the acquisition of H. pylori infection in Iran and also most studies did not pay attention to histopathological changes in stomach. Therefore, this study aimed to evaluate the role of breastfeeding in the acquisition of H. pylori infection in Iran and to compare the histopathologic changes occurring in children feeding on breast milk and in those feeding on formula. Subjects and Methods This is a case-control study carried out from March 2007 to February 2009. Participants consisted of children aged 2-14 years who were diagnosed with digestive symptoms, especially abdominal pain and undergone endoscopic survey and gastric biopsy in the Children’s Medical Center. Patients with a history of chronic debilitating disease were excluded and all cases and controls suffered mainly from abdominal pain but were in good general condition according to weight, history and absence of chronic disease stigmata. Children whose breastfeeding status was unknown or feeding consisted of a mixture of breast milk and formula were excluded from the study. The H. pylori infection was detected by Gimsa staining of the gastric biopsy and scored by Bor-shyang Sheu´s scoring[9]. Feeding practice was defined as breastfeeding exclusively in the first 6 months of life and formula feeding in this time period. Patients were placed in each group according to their history. We also conducted a pilot study in order to estimate the prevalence of formula consumption in Iran in infected and non-infected children by H. pylori, and discovered that in infected children 33.3% and in children who were not infected 14% consumed formula. We used these findings to determine the volume of our case and control groups. Hence, our case group consisted of 77 consecutive children infected by H. pylori and the control group consisted of 77 consecutive children not infected by this germ. We also asked the parents about their breastfeeding practices during the first 6 months after birth, the duration of breastfeeding period, the symptoms, and the duration of symptoms and concomitant diseases. In this study the Pearson's χ2 test and the Fisher's exact test were both employed to asses the relationship between H. pylori infection and variables such as age, gender, kind of feeding, duration of breastfeeding, symptoms and signs, duration of symptoms and signs, concomitant diseases, histopathologic changes in the stomach, concomitant histopathologic changes and the degree of H. pylori colonization. Statistical analysis was performed using SPSS 14 software (SPSS Inc., Chicago, IL, USA). Findings A total of 154 children were included in this study. From this sample, 77 children formed the case group (40 boys and 37 girls) and 77 the control group (42 boys and 35 girls). Children whose breastfeeding status was unknown or consisted of a mixture of breast milk and formula were excluded from the study. Table 1 and 2 show gender, mean age, kind of feeding, duration of breastfeeding, symptoms and signs, concomitant diseases, histopathologic changes in the stomach, concomitant histopathologic changes and the degree of H. pylori colonization in the case and control groups. A significant association was found between H. pylori infection and feeding with formula (P=0.04; Odd's ratio=2.92) and association of H. pylori infection and age (P=0.006). In case group, a significant difference was found between breastfeeding and the age of infected child (P=0.03), breastfeeding and duration of symptoms (P=0.02), and finally, breastfeeding and H. pylori colonization degree (Exact value=0.02). The more common gastric histopathologic changes in the case group were moderate gastritis (P=0.03), active gastritis (P=0.006) and follicular gastritis (P<0.001). More common histopathologic changes of stomach in control group were normal stomach (P<0.001) and mild gastritis (P=0.001). There was no significant difference between case and control group in the duration of breastfeeding (P=0.4), sex (P=0.7), type of symptoms, concomitant diseases (Exact value=0.5), duration of symptoms (P=0.7), severe gastritis (Exact value=0.12), peptic ulcer (Exact value=1), esophagitis (P=0.4), duodenitis (P=0.676), duodenal villous atrophy (P=0.4), Giardia infection (Exact value=1) and duodenal ulcer (Exact value=1). Discussion Acquisition of H. pylori takes place within the first five years of life[10] and can produce severe inflammatory and immune responses, chronic gastritis, duodenal ulcer and mucosa-associated lymphoid tissue (MALT). Even though breastfeeding has a protective effect on a variety of infant illnesses, it also has the potential to increase the risk for H. pylori infection by placing the breastfed children in close contact with the infected mother. Such paradoxical findings motivated us to specifically investigate the association between type of feeding in infancy (breastfeeding or formula) and H. pylori infection. Some studies have shown breastfeeding’s protective effect against the acquisition of H. pylori infection[1-4], while other studies have reported that breastfeeding does not have a protective effect against the acquisition of H. pylori infection[5-7]. Furthermore, these studies suggest that breastfeeding can even increase the rate of infection, especially in children breastfed for longer than 6 months[8]. This study was successful in determining the protective effect of breastfeeding history on H. pylori infection in children of Iran and was in parallel with Chak study in 2009[11]. The possible mechanisms enrolled in this protection may be the lactoferrin in human milk which binds to H. pylori liposaccharideinactivating the organism[12]. Also, Clyne et al showed that breast milk inhibits H. pylori adherence to gastric adenocarcinoma cell line in vitro[13]. One important point of our study is the evaluation of histological changes and separating their severity into two groups. This is not done in other studies. We showed that it is more common to see more severe gastritis and also more H. pylori organisms (more colonization) in gastric biopsies of formula fed children which may be due to lactoferrin effect as mentioned above or it may be due to H. pylori-specific IgA present in breast milk[14], which formula lacks. Our study had some limitations: it was conducted on a small sample of children suffering from digestive symptoms; therefore, the results might have been different if healthy children were taken into the study. Additionally, we used histopathologic changes in biopsy in order to evaluate H. pylori infection status in infants without having any knowledge regarding the H. pylori infection status of the mothers. Conclusion Our study reveals valuable information about the role of breastfeeding in protection against H. pylori infection. More specifically, it appears that breastfeeding in the first 6 months after birth may decrease the degree of colonization, postpone infection until older ages, shorten the duration of symptoms, and be concomitant with milder gastritis. As a result, we can recommend breastfeeding as a possible reliable method to prevent the consequences of H. pylori infection: gastritis, duodenal ulcer and lymphoma. It must also be mentioned, that breastfeeding may have a protective effect only in the first year of life and after that, it can increase H. pylori infection by facilitating mother-child transmission, especially if the mother doesn't have good hygienic habits. To achieve more accurate results, it is recommended to do similar studies on a larger sample, which includes both healthy and infected children. Acknowledgment The financial support of this study was provided by Tehran University of Medical Sciences. The authors have no competing interests. Conflict of Interest: None References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}
{kind=link}