 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 335-342 Incidence of Childhood Cancers in Golestan Province of Iran Abdolvahab Moradi1, PhD; Shahryar Semnani1 , MD; Gholamreza Roshandel*1, MD; Narges Mirbehbehani2, MD; Abbasali Keshtkar1, MD, PhD; Mohsen Aarabi1, MD, PhD; Abbas Moghaddami3 , MSc, and Fatemeh Cheraghali2, MD 1Research
Group, Golestan Research Center of Gastroenterology and Hepatology, Golestan
University of Medical Sciences, Gorgan, IR Iran Received: Nov 18, 2009; Final Revision: Feb 19, 2010; Accepted: Mar 30, 2010 Code Number: pe10050 Abstract Objective: This
paper presents the incidence rates of childhood cancers using the data
obtained from Golestan
population based cancer registry (GPCR) between
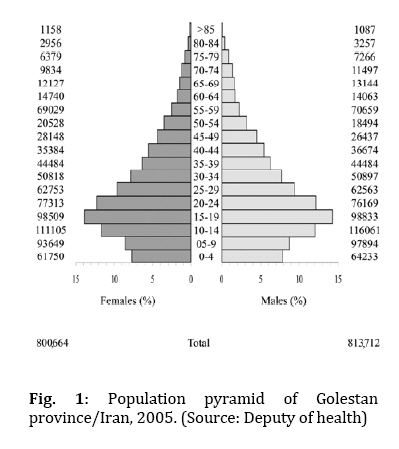
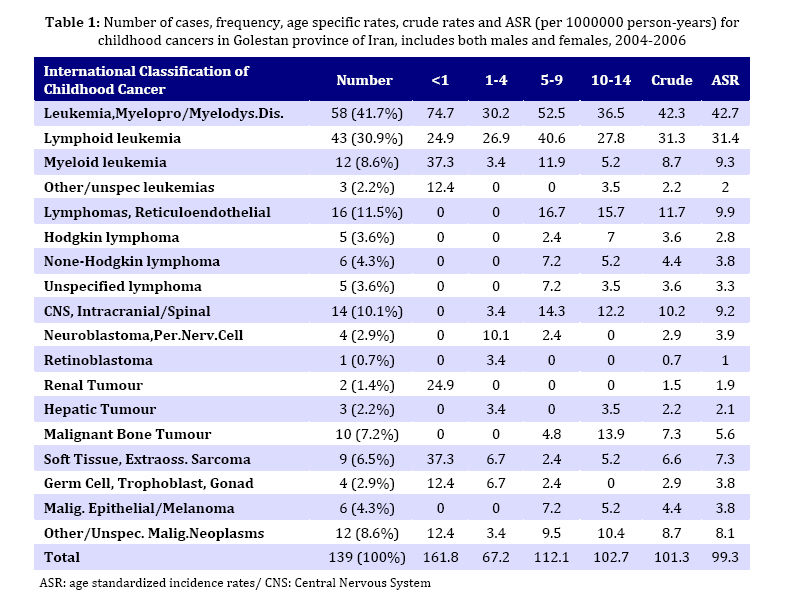
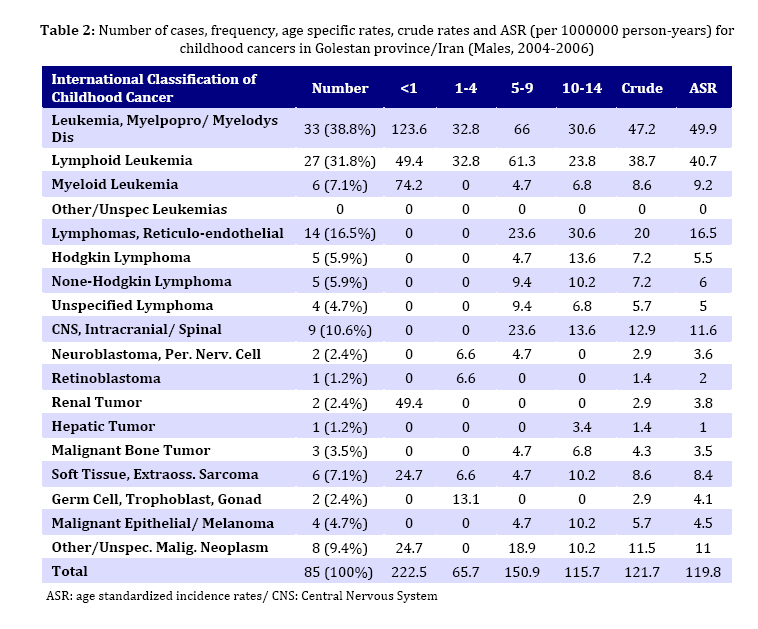
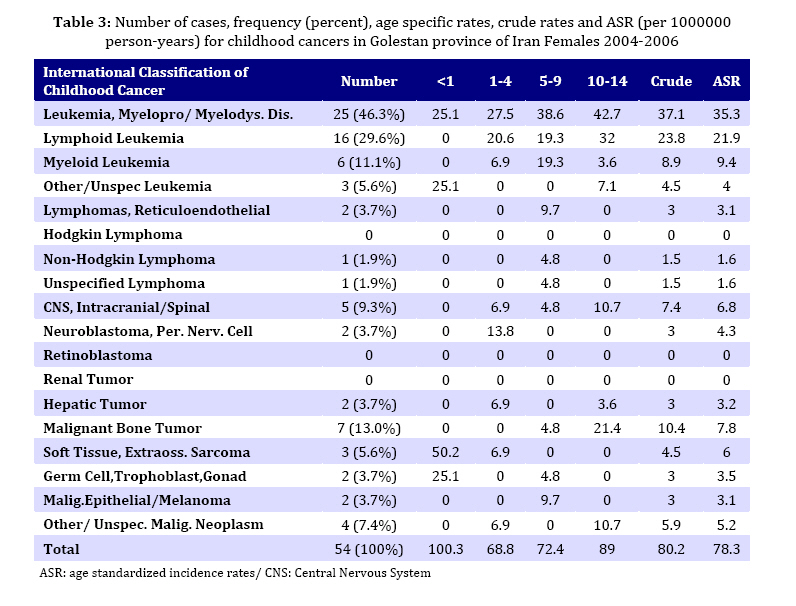
2004 and 2006. Key Words: Childhood; Cancer; Population; Leukemia; Cancer registry; Iran Introduction During the past century, the patterns of morbidity and mortality have changed dramatically in medium- and low-resource countries. That means chronic diseases, including cancers, have been emerged as one of the most challenging problems for public health systems in these countries. Cancer in children is rare, accounting for about one percent of all cancers. About 1 in every 600 children develops cancer before the age of 15. Still relatively little is known about its causes[1]. Despite its rarity and great improvements in treatment and supportive care, cancer is still the leading cause of death from disease in children younger than 15 years. It accounts second only to accidents in most age groups[2]. In the United States Cancer is the fourth most common cause of death after unintentional injury, homicide, and suicide among persons aged 1-19 years[3,4]. The American Cancer Society estimates that in the US in 2008, 10,730 children under fifteen years of age were diagnosed with cancer and 1,490 children died from the disease. Five-year relative survival from childhood cancer has increased markedly over the past 30 years, from less than 50 percent before 1970 to 80 percent now[5]. It accounts for 4% of deaths of children under 5 years of age and 13% for children 5–15 years of age in the Iranian population contributing to 15% of total loss of life in the under 15-year age group[6]. Childhood cancer is not a single disease. There are many different types. Compared with adult cancers they tend to have different histologies and occur in different sites of body[7]. The most common cancers in children are leukemia, central nervous system (CNS) tumors and lymphomas[8]. Common adult cancers such as lung, breast, colon, and stomach are extremely rare among children. On the other hand, some types of cancer are almost exclusively found in children, especially embryonic tumors which arise from cells associated with the fetus, embryo, and developing body. The first step in controlling the cancer burden is to collect information about the incidence, type, and location of cancers, and this is best done within the framework of cancer registries. In 1930 cancer registry has been concerned as an effective preventing and controlling tool for cancers. Registries may play an important role in research into the cause of cancer, both by providing data on patterns and trends, and in different types of epidemiological study (in particular, in their ability to follow up groups of persons exposed to potential hazards). They comprise an essential element in the planning and monitoring of cancer control strategies, and for identifying priorities in public health. As a result the first population based cancer registry unit covering data derived from whole country initiated in Denmark in 1942[10]. The first cancer registry conference based on population resources was organized in 1946[11]. In 1950 WHO set in a committee to support cancer registry programming[12]. In 1965, International Agency for Research on Cancer (IARC) was established in order to specify cancer related research topics by the world health organization (WHO) and in 1966 the International Association of Cancer Registries (IACR) started its work officially and published its first global report as "cancer in five continents''. For the first time in Iran, cancer related data was published by Dr Habibi in 1956[13]. Golestan province is one of the thirty provinces of Islamic Republic of Iran. It is located in southeastern edge of Caspian Sea (northeast of Iran). Up to now, many research groups were motivated to set cancer registration in this area but all of them were temporary and stopped their activity after a few years. So the necessity of collecting data about cancers had been sensed in this area. This was the main cause to motivate the officials of Golestan Research Center of Gastroenterology and Hepatology (GRCGH) in Golestan University of Medical Sciences (GOUMS) to fund and establish the Golestan Population-based Cancer Registry (GPCR). This was done in collaboration with the Digestive Disease Research Center (DDRC). The activity of the GPCR started in 2004 and was accepted as a voting member of the IACR in July 2007. This paper presents data on childhood cancers (aged 0-14 years) in Golestan province of Iran during 2004 to 2006. Subjects and Methods Type of study: This was a descriptive cross-sectional study. Golestan population: The most recent Iranian census was done in 2006 and plans are being made for the next census to take place in 2011. Provincial census of population data for years between the national censuses intervals is performed annually by health department of GOUMS. In this paper the data of provincial census was used to design the population pyramid of Golestan province in 2005 (Fig 1). Case definition: GPCR registered only primary cancers while additional tumors that result from the invasion or metastasis of cancers to other organs were not considered. Malignant tumors of all organs were registered based on the IACR standards. All cancer cases aged between 0-14 years at the time of diagnosis (during 2004 to 2006) were enrolled. Case finding: Data on newly diagnosed (incident) cancer cases were collected from all public and private diagnostic and therapeutic centers (hospitals, pathology/laboratory centers, imaging centers and some of the specialist physician's private offices) of the whole province. GPCR also had close collaboration with some of medical centers and regional registries outside the province to minimize loss of the data and consequent underestimation. Incidence data discussed in this paper are based on cases of primary cancers which were first diagnosed among Golestan residents from March 2004 to March 2007. Data collection: Two kinds of questionnaires, the first for outpatient and the second for inpatient cases, were used for data collection. Items collected in GPCR consisted of the patient's demographic particulars, anatomical site of the cancer, histology of tumor, method of diagnosis, date of diagnosis, method of treatment and outcome (date of death in case the patient has died). In some centers, data was collected passively ie, notifications of diagnosed cases were sent to the GPCR office on a routine, continuing basis. Thirty four health professionals underwent specific training for data abstraction in these centers. Data collection in other centers was active, the registry staff regularly visited them and collected information on newly diagnosed cancer cases. Ten percent of questionnaires were checked and compared with original documents in the source centers to verify accuracy and completeness of the abstraction process. For classification of the lesions the third edition of International Classification of Childhood Cancer (ICCC-3) coding system was used; it applied the rules, nomenclature and codes (morphology, topography, and behavior) of the third edition of the International Classification of Diseases for Oncology (ICD-O-3). IARC multiple primary rules[14] were used for patients with malignant tumors in more than one site. Ethical issues and confidentiality: Staffs of the registry was educated and asked to consider confidentiality in all stages of registry process including collection on notifications, transmission of information, access to and storage of data, use and release of data and record linkage. Confidentiality measures were used to ensure the preservation of anonymity of cancer cases, the best quality of registry data and the best possible usage of the data. Statistical analysis: Data were entered into CanReg-4 software[15], created and published by the IACR. Finally, numbers of cases by sex, age and primary site as well as age standardized incidence rates (ASR) (per 1000000 person-years) for cancers were calculated. By using the age standardized incidence rates (ASR), we controlled the differences in the age distribution of populations and consequently were able to carry out meaningful comparisons of cancer risk between the present results and other cancer registries. Findings Totally 5076 cancer cases (all ages) were diagnosed in GPCR during 2004 to 2006. Of these, 139 (2.74 %) were children (aged 0-14 years) with mean (±SD) age of 8.06 (±4.48) years. 61.2% of these cases were male and 66.19% lived in urban areas. Most of cases (42.4%) and least of them (9.4%) were in 10-14 and <1 year old age groups, respectively. The diagnosis in 82% of cases was based on microscopic verification (MV) and 7.2% on death certificate only (DCO). The other ones were diagnosed based of clinical data (4.3%) and para-clinical investigations (6.5%). Number of cases, frequency, age specific rates, crude rates and ASR (per 1000000 person-years) for childhood cancers in total children population, males and females are shown in Tables 1, 2 and 3 respectively. Discussion The most frequent childhood cancers in Golestan province were leukemia, lymphomas and CNS tumors (Table 1). The first three childhood cancers in males were the same as in the total population. But in females, leukemia, malignant bone tumors and CNS tumors were located on the top of childhood cancers. In United States, in 1995 the most common cancers in children were acute leukemia, CNS tumors, and lymphomas[8]. A study in Mexican republic reported the principal groups of neoplasm were leukemia, CNS tumors, and lymphomas[16]. In German Childhood Cancer Registry (GCCR) during 1980-2005 the three top cancers were leukemia, CNS tumors and lymphomas[17]. The results of surveillance epidemiology and end results (SEER) during 1975-95 showed that leukemia, CNS tumors and lymphomas were first three childhood cancers[18]. As mentioned above, the present results showed some differences with the results of other studies. This may be due to the specific conditions in Golestan province resulting in higher incidence of lymphoma in comparison with CNS tumors. Another explanation for this difference is under-reporting of CNS tumors because of diagnostic difficulties. Finally it should be considered that here we reported the first three-year results of the GPCR and of course underestimation is a usual limitation of newly established cancer registries. Further studies are needed to determine the actual reasons of the above mentioned difference. The incidence rates of malignant bone tumors, neuroblastoma and hepatic tumors were higher in females than in males. Other cancers were more frequent in males. According to the present findings, in Golestan province, ASRs of leukemia were 42.7 per million in total pediatric population, 49.9 in males and 35.3 in females, during 2004-2006. SEER reports showed that in the years 1975- 1995 the ASRs of leukemia were 43.8, 47.4, and 40.1 per million in both sexes, males and females, respectively[19]. These results were close to the results of Golestan province. In another study in Mexican republic during 1998-2000 the ASR of leukemia was 55.4, 58.2 and 49.9 per million in total children population, males and females, respectively[16]. In this study, ASRs of lymphomas were 9.9, 16.5 and 3.1 per million in both sexes, males and females, respectively. The ASRs of Hodgkin and non-Hodgkin lymphoma were 2.8 and 3.8 per million. Based on SEER reports the ASRs of Hodgkin and non-Hodgkin lymphoma were as high as 5.5 and 8.6 per million in total children population during 1990-95[20]. A study in Mexican republic showed that, ASRs of lymphomas were 20.8 and 8.6 per million in males and females, respectively[16]. In the present study, CNS tumors were the third common cancers diagnosed in both genders. According to SEER reports the ASR of CNS tumors in the USA during 2004-2007 (27.4/1000000) was considerably higher than ours (9.2 per million)[21]. As mentioned above, this may be due to the specific conditions of Golestan province or as a result of under-reporting of these tumors. As seen in Table 2 and 4 the ASRs of CNS tumors were 11.6/1000000 in males and 6.8/1000000 in females. Arturo Fajard et al in Mexican republic reported the ASRs of CNS tumors as high as 14.4, 16.2 and 16.9 per million in total children population, males and females, respectively[16]. General reports from different parts of the world indicate that leukemia is the most predominant cancer type in children. The second common cancer type was lymphoma in Golestan Province followed by CNS tumor types. This was different in other regions. The reports from some countries such as Costa Rica, Malaysia (males) and China are similar to the results of the present study[22,23]; but in other parts leukemia is followed by CNS tumors. It means that lymphomas ranked as the third common cancer type and the second one was CNS tumors. This had been reported in countries such as USA (whites and blacks), Costa Rica, Israel, India, Japan, Great Britain, Australia, Brazil and Malaysia. CNS tumors in some regions as in above countries are more than two folds in comparison with lymphomas[23]. Here we could not retrieve stages of the cancers and related survival rates, thus other detailed researches are suggested to follow cases diagnosed with children's cancers and to assess the related risk factors between males and females in different age groups. Conclusion Leukemia was the most common childhood cancer in Golestan province of Iran. Lymphomas and CNS tumors were the second and third ones, respectively. The incidence rates of these cancers were relatively high in Golestan province. So, childhood cancers should be mentioned as an important issue in health policy making in Golestan province of Iran. Acknowledgment The authors thank Professor Reza Malekzadeh and Dr Alireza Sadjadi for their supports. We also wish to thank Dr Azadehsadat Zendehbad, Mr Khodaberdi Kalavi, Dr Seyed Mehdi Sedaghat, Dr Rashid Ramazani, Dr Elham Dabiri, Mrs Honeyehsadat Mirkarimi, Mrs SeyedZinab Hasheminasab, pathologists, physicians and other health professionals in Golestan province for their valuable helps and efforts. The protocol was approved by the regional ethics committee. This work was supported by Golesran Research Center of Gastroenterology and Hepatology, Golestan University of Medical Sciences and Digestive Diseases Research Center, Tehran University of Medical Sciences. Conflict of Interest: None References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}
{kind=link}
{kind=link}
{kind=link}