 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 343-347 Infection Rate of Cryptosporidium parvum among Diarrheic Children in Isfahan Hossein Saneian1, MD; Omid Yaghini1, MD; Amene Yaghini2, MD; Mohammad-Reza Modarresi1, MD, and Mohsen Soroshnia2, MD 1Department
of Pediatrics, Isfahan University of Medical Sciences, Isfahan, IR Iran Received: May 15, 2009; Final Revision: Feb 19, 2010; Accepted: Apr 21, 2010 Code Number: pe10051 Abstract Objective: Cryptosporidiosis
is an important enteric parasitic infection among infants and children
in developing countries with significant morbidity and mortality especially
among immuno-suppressed individuals. The aim of the present study was
to estimate the prevalence of enteric cryptosporidiosis in children presenting
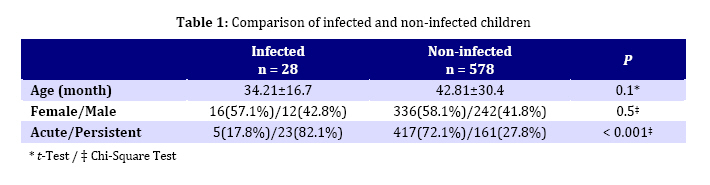
with diarrhea in Isfahan. Key Words:Cryptosporidiosis; Cryptosporidium parvum; Diarrhea; Gastroenteritis; Prevalence Introduction Diarrhea, including that of parasitic origin, remains one of the most common illnesses among children and, as reported by the World Health Organization, is one of the major causes of infant and childhood mortality in developing countries[1]. Intestinal opportunistic parasitic infections are important causes of diarrhea which is a serious health problem in tropical regions. Giardia spp. and Cryptosporidium spp. are common parasitic causes of human diarrhea with the prevalence rate of 1%-3% in the industrialized world and 4%-17% in developing countries[2]. In developed countries, massive Cryptosporidium food borne and waterborne outbreaks have been reported because Cryptosporidium oocysts are not killed by conventional disinfectants and chlorination[3]. In developing countries, Cryptosporidium affects mostly children under five years of age and has been reported to be more common in malnourished than in well-nourished children[4,5]. C. parvum, a protozoan parasite of the phylum Apicomplexa, is an enteric pathogen that causes an acute as well as chronic diarrhea in humans. The human host range is broad and includes people with immunodeficiency, children in developing countries, and outbreaks among immuno-competent individuals[6]. In a healthy adult, infection often results in a self-limited diarrheal illness, however, in children of developing countries, cryptosporidiosis can result in persistent diarrhea leading to malnutrition and developmental delays[6]. Indeed, Cryptosporidium is still an under-diagnosed cause of diarrheal illness in children. Few reports with relatively small sample sizes are available on the prevalence and clinical presentation of Cryptosporidium infection in both immuno-compromised and immune-competent children in Iran[7-13]. The purpose of this study was to determine and compare the prevalence of C. parvum infection in children with an acute or persistent diarrhea in Isfahan city, central Iran. Subjects and Methods This cross-sectional study was prospectively conducted in three university hospitals in Isfahan from August 2007 to June 2008. Children aged one month to 10 years presenting with acute or persistent diarrhea were visited in each hospital by one of the researchers (pediatrician) of the study and were included consecutively. Diarrhea was defined as the passage of abnormally liquid or unformed stools at an increased frequency and further defined as acute if lasted <2 weeks and persistent if lasted for 2 to 4 weeks before admission[14]. Children who had used antiparasitic or antibiotic drugs before admission and also those with known hematologic diseases and immuno-compromised children were excluded from the study. Assuming the average prevalence of C. parvum to be 5% according to previous reports[12], and a margin error of 2% (difference between estimated and reported prevalence) and 95% confidence, a sample size of 456 was calculated for determining the overall prevalence of C. parvum. Fecal samples were collected in sterile plastic bottles and were transported without preservative and arrived in the central laboratory of Isfahan city within 24 hours of collection. The oocyst of C. parvum was tested using a modified acid-fast staining method which is a sensitive and specific approach for the identification of Cryptosporidium and coccidian oocysts in stools[15]. In this technique, the oocysts appear as pink to red, spherical to ovoid bodies on a blue or purple background. All samples were evaluated by a single experienced parasitologist. The study protocol was approved by the Ethical Committee of Isfahan University of Medical Sciences and consent was obtained from the parents. Data analysis was done using SPSS for Windows Version 16.0. The Chi-Square test was used to compare relative frequency of Cryptosporidium infection between children with acute and persistent diarrhea. Independent t-Test was used to compare the mean age between infected and non-infected children. Statistical significance was set at P<0.05. Findings During the study period, 606 children aged one month to 10 years were presented with acute or persistent diarrhea to three university hospitals in Isfahan. There were 254 (41.9%) males and 352 (58.1%) females with the mean age of 42.4±30.0 months. Acute or persistent diarrhea was present in 422 (69.6%) and 184 (30.4%) of the children, respectively. Total number of Cryptosporidium oocyst positive specimens was 28 (4.6%). Cryptosporidium oocysts were detected in 12.5% (23/184) of the children with persistent compared to 1.2% (5/422) of the children with acute diarrhea; P<0.001. Most (89.2%) of the infected children were under 5 years of age, however, the age difference between the infected and non-infected children was not statistically significant; P=0.1. Also, there was no significant sex difference between the infected and non-infected children; P=0.5 (Table 1). The age difference between children with acute and persistent diarrhea was not statistically significant (43.9±33.4 vs 38.9±19.6 months, P=0.06) and there was no significant difference between the two sexes (248/174 vs 104/80 female/male ratio, P=0.6). Discussion Intestinal parasites are very common in developing countries and Cryptosporidium has revealed to be one of the most common parasites. Cryptosporidium infests the small intestinal epithelium, thereby, results in an accelerated loss of villous enterocytes, leading to severe villous atrophy and a malabsorptive and secretory diarrhea which is the most pronounced clinical feature of the infection. Other symptoms include dehydration, weight loss, stomach cramp, or pain, fever, nausea, and vomiting[6]. The infectious dose is low and feeding studies have demonstrated that the ingestion of as few as 10-30 oocysts can cause infection in healthy persons[16]. Infected persons have been reported to shed 108-109 oocysts in a single bowel movement and to excrete oocysts for up to 50 days after cessation of diarrhea[16,17]. There are discrepancies in the prevalence of cryptosporidiosis in children among surveys in different parts of Iran. The reported prevalence is from 1.5% in Rasht (northern city of Iran) to 21.4% in Shiraz (southern city of Iran)[7-13]. Our analysis confirmed that cryptosporidiosis is a common infection in children of our community. The difference in the reported prevalence may be attributed to differences in study population (considering age range), diagnostic methods, environmental risk factors (public water supply), time of the study (summer vs winter), nutritional status of the children, and other risk factors[6,18,19]. Educational level of parents has also been reported as a risk factor[18]. In other countries, the rates of cryptosporidiosis are 1%-2% in Europe, 0.6%-4.3% in North America, and 3%-10.2% in Asia, Australia, Africa, and Central and South America[20]. Several methods are available for identification of Cryptosporidial oocysts in fecal specimens including modified acid-fast staining which detects oocyst wall, fluorescein-conjugated monoclonal antibody-based detection of oocyst wall antigen, enzyme-linked immunosorbent assay (ELISA) which detects Cryptosporidial antigen and most recently polymerase chain reaction (PCR) which detects Crytosporidial DNA[6]. Modified acid-fast stain of a fecal smear has been the gold standard for detecting Cryptosporidium oocysts in stool. This method is commonly used in clinical microbiology laboratories to easily identify Cryptosporidial oocysts. Although the concentration and staining procedures are time- consuming and also require an experienced microscopist to read the slides, it is inexpensive and allows the detection of other parasites (eg, Isospora and Cyclospora) at the same time. However, the sensitivity for the detection of Cryptosporidium is substantially better with ELISA formats or immunofluorescent assays[6]. PCR method is sensitive, but the cost and tedious methodology have limited its use in the clinical microbiology laboratory. Regardless of the method used, it is extremely important that the physician remembers to request Cryptosporidial testing when stool from a child with diarrheal illness is to be examined for ova and parasites[6]. The results of the present study showed that children with cryptosporidiosis are more likely to present with persistent diarrhea, compared to acute diarrhea. In a report from southeastern Iran, Hamedi and colleagues also found that diarrhea lasted significantly longer in children infected with Cryptosporidium[11]. However, Khalili and colleagues in their study on 171 children found no relationship between type of diarrhea and infection[10]. Although our study did not show significant age difference between the infected and non-infected children, most of the infected children, as expected, were below 5 years old. Though humans are susceptible at any time in their lives, the prevalence of cryptosporidiosis is higher in younger children mostly in children aged below 5 years[8,10,11]. The occurrence of high infection rates in younger children might be attributed to their weak immune responses and/or risk of contact with the oocysts. However, more studies are needed to confirm this subject[12,18]. There are some limitations for the present study. Although the sample size of the study was large enough, sampling was consecutive and not random. However, the study was multicenter and we conducted the study through one year, so it is unlikely that season or selection bias affected our results. Also we applied the modified acid-fast staining and although it is a sensitive and specific approach for the identification of Cryptosporidium, ELISA and immunofluorescent assays are more sensitive in this regard. We recommend evaluating children for important risk factors for infection with Cryptosporidium, such as nutritional and socioeconomic status, for future studies. Conclusion The prevalence of Cryptosporidiosis in children presenting with persistent diarrhea is considerable and we suggest routine stool examination for Cryptosporidium in these children for early diagnosis and treatment to prevent possible complications. Also, for control and prevention of this infection, strengthening water quality standards and improving sanitary practices are required. Acknowledgment This study was supported by a grant from the Vice Chancellor of Research, Isfahan University of Medical Sciences. We would like to thank Dr Ali Gholamrezaei for editing the manuscript. Conflict of Interest: None References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}