 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 348-352 Is There Any Association between Spina bifida occulta and Primary Vesicoureteral Reflux? Mehrzad Mehdizadeh1,2, MD; Azadeh Roohi2, MD; Mohsen Hemami3, MD, and Seyed-Taher Esfahani2,4, MD 1Department
of Radiology; Tehran University of Medical Sciences, Tehran, IR Iran Received: Jul 26, 2009; Final Revision: Dec 08, 2009; Accepted: May 10, 2010 Code Number: pe10052 Abstract Objective: Spina
bifida occulta (SBO) has been largely considered a benign entity without
clinical significance; however, there has been dispute among various
authorities, and some believe that the lesion may be linked with various
neurologic conditions like urologic dysfunctions. Vesicoureteral reflux
(VUR) and lower urinary tract dysfunction are closely related. We examined
whether the existence of SBO is related to the prevalence and severity
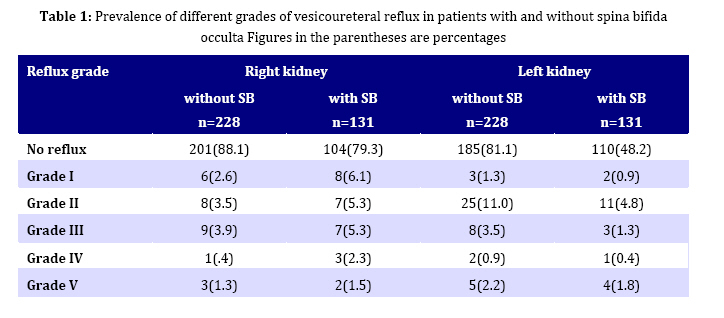
of VUR in children. Key Words: Spina Bifida Occulta; Vesico-ureteral reflux; Voiding dysfunction; Spinal anomalies Introduction Spina bifida is a disorder in which two sides of vertebral arches, usually in lower vertebrae, fail to fuse during development resulting in an open vertebral canal. There are two types of spina bifida: 1) The commonest type is spina bifida occulta (SBO), in which there is a defect in the vertebral arch of L5 or S1, and results in failure of posterior arch to fuse in the midline. 2) The more severe form of spina bifida vera cystica involves complete failure of fusion of posterior arch at the lombosacral region with a large outpouching of the meninges. This may contain cerebrospinal fluid (meningocele) or a portion of spinal cord (myelomeningocele). These abnormalities may result in a variety of neurologic defects including impaired walking and bladder function[1,2]. The reported frequency of occurrence of SBO varies widely, depending largely on the age group included in a particular study[3,4]. Although it is true that this lesion is present at birth, some cases seem to vanish with increasing bone maturity. It should be kept in mind that in normal conditions, the two halves of the posterior arch fuse between the ages of 5 and 8 years. Studies with children have indicated that an apparent SBO defect that persists past the age of 8 years may fill with new bone as a part of the aging process, ossifying, in fact a radiologically undetectable connective tissue matrix in the posterior arch. To obtain a true sense of the prevalence of this lesion, one must examine its frequency of occurrence in relation to chronologic age. In <18 year age groups, the incidence may be as high as 50%. The true prevalence of this anomaly, excluding cases that later disappear, has been estimated at approximately 17% of examined spines[3,5]. Spina bifida vera is associated with variety of neurologic dysfunctions in lower urinary tract, but SBO often is asymptomatic and is considered of no clinical significance[6,7]. However, it has been implicated in the etiology of urinary voiding problems[8-10]. Vesicoureteral reflux (VUR) and lower urinary tract dysfunction are closely related[11-14]. Bladder dysfunction may have an etiologic role in development of VUR or may aggravate it[11,12]. Treatment of bladder dysfunction increases spontaneous resolution of VUR[13]. Primary VUR generally improves with time[14]. So both conditions are more common in infancy and may resolve with increasing age and both may be related to the voiding dysfunction. Herein we studied if there is a relation between SBO and primary VUR in children. Subjects and Methods We investigated 359 children after the first attack of febrile urinary tract infection that had been referred to radiology department for obtaining voiding cystourethrography (VCUG). After treatment of infection, with written order of their physicians and permission of parents all underwent a standard VCUG to detect VUR and other lower urinary tract anomalies. Reflux grading was done according to the international classification of the reflux[15]. In each patient presence or absence of SBO, and if SBO was present, its location was determined with KUB or post-voiding films. SBO was diagnosed by hypoplasia or aplasia of the spinous process, producing a radiolucent defect on anteroposterior KUB or postvoiding films. Children with neurologic bladder or with other spinal anomalies were excluded from the study. SPSS software version 16.0.2 (SPSS Inc., Chicago, IL), was used for data analysis. To compare frequency of variables between groups Chi-square and for detecting trend, a trend Chi square were used. P value lower than 0.05 was considered significant. This study was approved by the ethics committee of the Tehran University of Medical Sciences. All radiographs were taken with written order of responsible physicians. The nature and purpose of performing VCUG was explained and verbal consent taken from parents before radiography. Findings Three-hundred fifty nine children (128 boys and 231 girls), 2-14 years old (mean age 75±37 months), were evaluated. Of 359 children 228 (63.5%) had normal spines and 131 (36.5 %) had SBO. The location of SBO was: L5 6 (0.045%) cases, L5-S1, 47 cases (35.9%), S1 78 (59.5 %) cases. Of 228 children with normal spines 174 (76.3%) had no VUR and 54 (23.7%) had VUR. Of 131 children with SBO, 91 (69.5%) had no VUR and 40 (30.5%) had VUR. The prevalence of VUR between children without SBO and children with SBO was not significant (P=0.15). Among children with SBO in L5, 16.7%, in L5-S1 38.3% and in S1 26.6 had VUR. There was no significant relation between location of SBO and prevalence of VUR (P=0.4). We also evaluated if there was a relation between presence of SBO and severity of VUR. The VUR grades in both kidneys are shown in Table 1. There was no significant difference or trend between presence of SBO and severity of reflux (Chi2 for trend). Discussion SBO is a common anomaly[3-5]. Fidas et al reviewed plain radiographs of the urinary tract on 2707 normal adult volunteers. This condition was twice as common in males as in females and was commoner in young adults[3]. The commonest defects were either in S1 alone or involved S1 and S2 together. Isolated defects of L5 or S2 were rare. The incidence of SBO decreases with age, possibly as a result of new bone formation or calcification[4,5]. According to Sutow and Pryde the incidence of SBO diminishes in male from 22% in the seventh year to 4% in adults, and in females from 9% in the seventh year to 1% in adults[4]. The spina bifida vera cystica is well known and has undisputed neurologic sequelae, but most individuals with SBO are asymptomatic and lack neurologic signs and the condition is considered of no clinical significance[6,7]. However, SBO is linked with a variety of functional disorders of lower urinary tract in children[8-10]. Sakakibara et al performed uroneurologyic assessment of patients with spina bifida cystica and occulta. Their study showed that SBO presents with a wide spectrum of urodynamic abnormalities including upper and lower neuron types of bladder and urethral dysfunction. In some of their SBO patients urinary symptoms like nocturnal enuresis were the sole initial complaints and had no other neurological abnormalities[8]. In contrary, Samuel and Boddy evaluated 158 children presenting with lower urinary tract and bowel dysfunction for associated spinal abnormalities. They concluded that SBO in these children is probably a coincidental finding and its significance in this cohort is not established[16]. Also, Nejat and co- workers showed that there is no significant association between SBO and functional bowel and urinary problems[17]. So, there are conflicting reports regarding the relation between SBO and functional disorders of urinary tract. Probable role of SBO as a finding associated with spinal cord dysfunction remains unclear. Miyazato et al reported that the location of SBO predicts the outcome of treatment for primary nocturnal enuresis in children, in their study patients with L5 and L5-LS1 spina bifida were less responsive to treatment compared to patients with sacral SBO[9]. In contrary, Kumar et al studied incidence of SBO in nocturnal enuresis cases and compared outcome of enuresis in children with or without SBO. They found that outcome of patients with SBO is not different from those without SBO[18]. Ritchey et al reviewed retrospectively 456 patients with diurnal enuresis to determine the relationship between spina bifida occulta and attainment of continence. They compared urodynamic findings in children with or without SBO. Findings on urodynamic studies were similar in both groups. Also, the outcome for enuretic children with SBO was comparable to those with normal spines[19]. VUR and lower urinary tract dysfunction are closely related. There are reports showing that lower urinary tract dysfunction is a factor in pathogenesis of VUR[11,13] and treatment of voiding dysfunction prompts resolution of VUR[13]. Because both SBO and VUR may be related to voiding disorders, we proposed that there may be a relation between these two disorders, but our study showed that SBO or its location has no relation with prevalence or severity of VUR. The SBO is subject of dispute among various authorities, with one faction adamantly refusing to accept the premise that the lesion may be linked with various neurologic conditions and the opposing side insisting that a plethora of abnormalities may be associated with the condition[5]. Conclusion In our study, the prevalence of VUR between children without SBO and children with (isolated) SBO was not significant (23.7% vs. 30.5%). In addition, there is not any association between presence and location of (isolated) SBO and severity of primary VUR. Acknowledgment This research was approved by Pediatrics Department Research Committee in Tehran University of Medical Sciences. Conflict of Interest: None References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}