 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 353-357 Diphallus: Report on Six Cases and Review of the Literature Ali-Reza Mirshemirani, MD; Naser Sadeghyian, MD; Leila Mohajerzadeh, MD; Hojat Molayee, MD, and Parand Ghaffari, MD Pediatric Surgery Research Center, Mofid Children's Hospital, Shahid Beheshti University of Medical Sciences, Tehran, IR Iran Received: Oct 22, 2009; Final Revision: Dec 11, 2009; Accepted: Feb 16, 2010 Code Number: pe10053 Abstract Background: Diphallus
is an extremely rare anomaly. Numerous associated genitourinary, gastrointestinal
and other anomalies have been described with diphallus. These patients
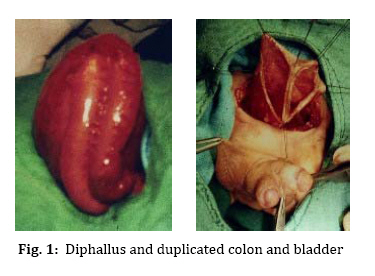
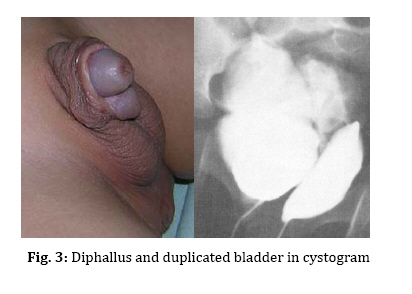
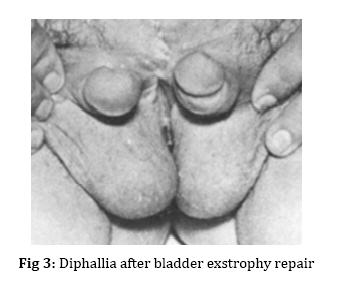
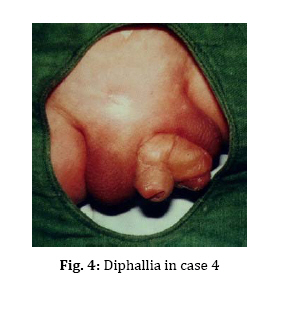
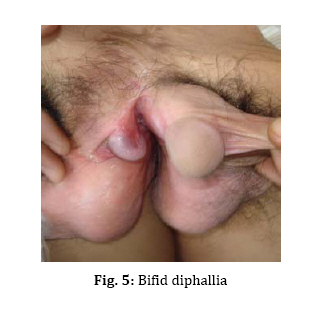
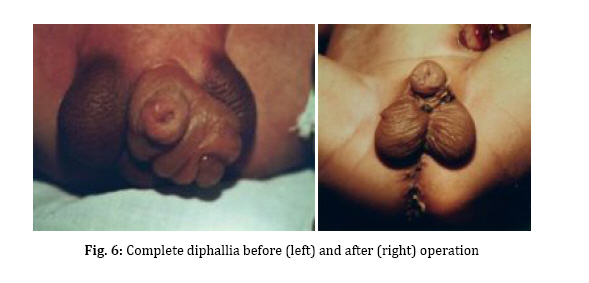
need several investigations, and finally surgical intervention. Key Words: Diphallus; Urethral duplication; Reconstructive surgical procedures Introduction Duplication of the penis or diphallus is a rare anomaly that occurs once in every 5 to 6 million live births [1]. Approximately 100 cases have been reported since the first case reported by Wecker in 1609[2]. Neugebauer in 1898 and Nesbit and Bromme in 1933 reviewed cases in the literature [3,4]. The extent of duplication and the number of associated anomalies vary greatly, ranging from a double glans arising from a common shaft with no other anomaly to complete duplication of the phallus accompanied by multiple anomalies, such as ectopic scrotum, bifid scrotum, hypospadias, imperforate anus, bladder exstrophy, colon duplication, double bladder, and vertebral deformities [5]. Embryologically a diphallus deformity arises from either "separation" of the pubic tubercle, wherein each phallus will have only one corporal body and urethra, or "cleavage" of the pubic tubercle wherein each phallus will have two corporal cavernous bodies and urethras [6]. Diphallus has been classified in different ways, such as glandular, bifid, concealed, complete, hemidiphallus and triple penis [7]. Schneider classified diphallus in three groups: diphallia of glans alone, bifid diphallus, complete diphallia, and recently a fourth category of pseudodiphallia has been added [7]. The majority have a single corpus cavernosum in each organ [8]. Duplicated urethras usually may be associated with diphallus[9]. We herein discuss our six diphallic patients and associated anomalies. Patients were classified according to Scheneider classification: (glans diphallia, bifid diphallia, and complete diphallia). We evaluated also meatus type, scrotum and testis position. Finally surgical intervention was carried out to reconstruct diphallus and associated anomalies. Cases Presentation During 20 years, 6 cases of diphallus have been admitted in our department. The age of patients was between 2 days and 14 years. Five patients had complete diphallia and one had bifid diphallia. Meatus was normal in 3, hypospadiac in 2 patients and epispadiac in one patient. The most common associated anomaly was bifid scrotum (5 cases), and other anomalies consisted of duplicated bladder (3 cases), imperforate anus (2 cases), and hypospadias (2 cases). Phalloplasty was performed for all but one patient who was planned for future. All associated anomalies were also repaired. In the following, patients are described separately: Case 1: This 2-day old neonate with 2500kg body weight presented for evaluation of complex genitourinary and ano-rectal malformation. Physical examination revealed imperforate anus, complete diphallia, hypospadias and normal testes but bifid scrotum. Meatuses could be seen on both glanses. The first procedure done on the patient was a loop colostomy, which showed duplication of recto-sigmoid colon (Fig 1). Patient's karyotype was 46XY. Abdominal ultrasonography (US) showed normal kidneys and ureters but duplicated bladder. A cystogram with retrograde filling through both urethras demonstrated two bladders without reflux and no connection between them (Fig. 1). Table 1 shows more specific information on this patient. Case 2: The four-year old boy was admitted in our hospital for uro-genital evaluation. He was the product of a full-term pregnancy without complications. Birth weight 4kg. On examination he had diphallia with normal meatuses (Fig. 2). The scrotum appeared to be normal and contained one testis in each side. The karyotype was 46XY. US and cystography showed two independent bladders lying side by side and each one emptied through a separate urethra (Fig. 2). Hernia repair and cysto- urethro-phalloplasty were performed in two stages. Case 3: This 12-year old boy, one of four children in a family, was referred to our clinic for diphallus and inability for normal urination. He had a history of bladder exstrophy operation during neonatal period and infancy in another hospital. He had a 46XY karyotype. Physical examination revealed complete diphallus, neither of which had a meatus, scrotum was bifid and contained normal sized testes (Fig. 3). Radiographic study of different organs revealed lumbo-sacral hemivertebrae. Intravenous-pyelography (IVP) and kidney scan showed a single kidney, with extravasated dye over the phalluses. Cystography revealed a small bladder. Cecco-Vesical Augmentation and Mitrofanoff operation was performed in one stage. Now he is under observation with medical therapy. We plan to perform urethro-phalloplasty later. Case 4: This 1-year old boy presented with complete diphallus. On physical examination he had normal meatus on each phallus; scrotum was bifid and contained normal sized testes. Karyotype was 46XY. He had no prior history of operation and disease. IVP showed normal kidneys and ureters. On US and retrograde cystourethrogram he had two separate bladders, without any interconnection. Thus, complete duplication of bladder and urethra was diagnosed (Fig. 4). Cystophalloplasty was performed and excision of accessory bladder and urethra undertaken. Scrotoplasty was also carried out. Case 5: A 14-year old boy, the last of six children from an economically poor family. He had a history of difficult delivery and hypoxia. He was Referred to our clinic because of abnormal external genitalia. On examination he was hyperactive with abnormal behavior and neurological defects. He had complete bifid diphallia with one normal and another hypospadiac meatus, scrotum was bifid and contained normal testes (Fig. 5). US, IVP, voiding cystourethrography (VCUG) revealed normal kidneys, ureters and bladder but duplicated urethra, which was normal in the left but hypospadiac in the right side. His karyotype was 46XY, so the right hypospadiac phallus was excised and the left normal one repaired. Case 6: This 9-month old boy was referred to our clinic for urogenital abnormalities and imperforate anus. Body weight was 7kg. Karyotype was 46XY. He had a history of colostomy due to ano-rectal malformation in Another center. Physical examination revealed a well baby with complete diphallus, both sides' normal meatuses, bifid scrotum, normal sized testes, imperforate anus and divided colostomy. U/S, IVP, VCUG and ureterography showed normal kidneys, ureters, bladder and other organs, but duplicated urethra and ended loop rectum. Distal cologram showed narrow fistula to right sided urethra. Posterior sagittal ano-recto-plasty (PSARP) was performed, and one month later right phallus was excised and scrotoplasty carried out (Fig. 6). He is now in good condition and follow-up. Discussion Duplication of the penis or diphallus is a rare anomaly. Within 20 years we could find only six patients in our medical records. Diphallus may happen in clitoris which is also very rare, as Reported by Jeffcoate[10], but we did not have any in our series.Scheneider classified diphallus in three groups: diphallus of glans alone, bifid diphallus, and complete diphallus. Vilanova and Raventos have added a fourth category called pseudodiphllia[11]. We had five complete and one bifid diphallia in our series but no glans diphallia, Mutlu et al had no complete diphallus in their cases [6]. In our group 5 cases had a single corpus cavernosum. The meatus may be normal, hypospadiac, or epispadiac. In our study we had normal type in 3 cases, epispadiac in one case and hypospadiac type in 2 patients. Abdulkadir has reported on hypospadiac type[7]. The scrotum may be normal or bifid, our patients had bifid scrotum in 5 cases and only one patient had normal type. Priyadarshi has reported a case of bifid scrotum[8]. Associated congenital anomalies are present in the majority of cases. In our study we had bifid scrotum, hypospadias, duplicated bladder, imperforate anus, bladder exstrophy, colon duplication, inguinal hernia and kidney agenesis. This is different in reported cases [12, 13, 14]. Intestinal anomalies are mostly associated with complete diphallia, and imperforate anus[10,15]. We had only one case of this combination in our series. There are multiple embryological explanations for diphallus; we could not find any exact etiological factor in our study. Treatment of diphallus usually includes excision of the duplicated penile structure and its urethra. Associated anomalies can also be repaired surgically[2,15,16]. Conclusion All the patients with penile duplication (diphallus) have to be evaluated carefully because of the high incidence of other systemic anomalies and all can be repaired surgically. Acknowledgment The authors would like to thank Mrs. Saeedi for kind help to type and prepare this manuscript References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}