 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 3, July-September, 2010, pp. 363-366 Association of Sudden Death and Seizure with Left Ventricle Non-compaction in a Family Arman Masihi Kocharian1,2, MD; Ahamd Gamei Khosroshahi2, MD; Elahe Malakan-Rad1,2, MD, and Behzad Mohammadpour Ahranjani 2, MD 1Department
of Pediatrics, Tehran University of Medical Sciences, Tehran, IR Iran Received: May 11, 2009; Final Revision: Nov 14, 2009; Accepted: May 06, 2010 Code Number: pe10055 Abstract Background: Left
ventricle non-compaction (LVNC) or persistence of spongy myocardium
is a rare form of congenital cardiomyopathy which presents with cardiac
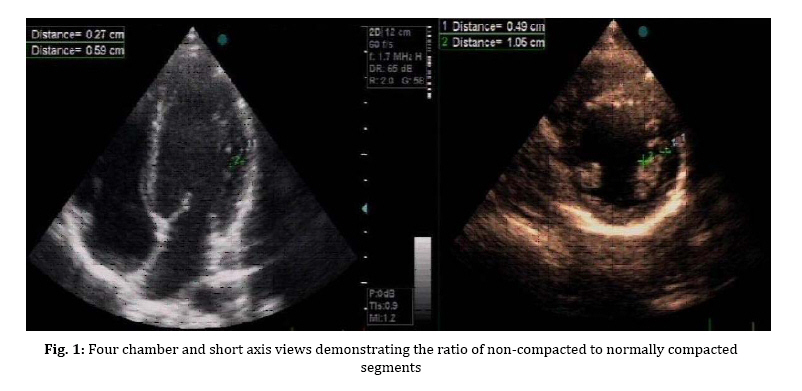
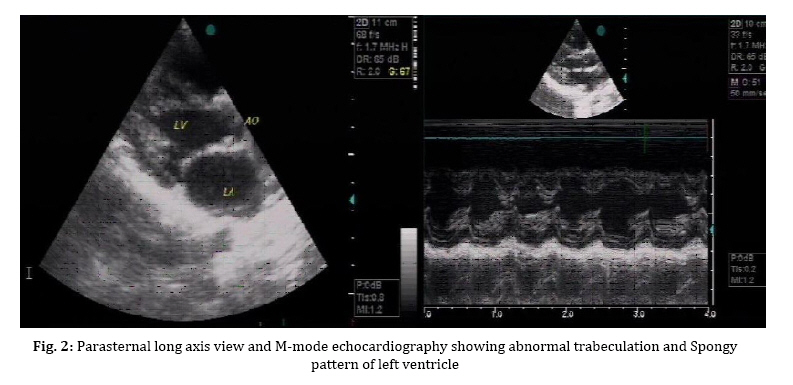
failure, thromboembolic events, arrhythmia and sudden death. Key Words: Cardiomyopathies; Non-compaction of the Ventricular Myocardium; Sudden death; Syncope Introduction Isolated left ventricular non-compaction (LVNC) is one of the rare genetic heart diseases recently known, and characterized by heterogeneous defects in endocardium accompanied by increased trabeculation due to abnormal embryogenesis of the normal myocardium. In this disease, the myocardium is composed of two layers: spongy or non-compacted and normal or compacted ones[1]. The pattern of heritage of LVNC is autosomal dominant and X-liked. The clinical manifestations include symptoms and signs of left ventricular failure (common), those of right ventricle (rare), ventricular arrhythmias, sudden death, mural thrombi and embolic events with cardiac origin[2]. No pediatric sudden death due to LVNC has ever been reported. We report a family having the history of two offspring deaths, at the ages of 9 and 16, with two live ones suffering from LVNC. Case Presentation We reported sudden death of a 9-year old boy with a history of two episodes of unprovoked convulsion and syncope in school and his 16-year old sister due to sudden death while she was getting back home after a feast. A 12–year-old boy and a 7-year-old girl were referred to pediatric cardiology clinic for cardiac evaluation following occurrence of sudden death in their siblings. He was born to consanguineous parents. The first pregnancy of the mother ended in abortion at the age of two months of gestation, and the second offspring was a girl who died one week after birth following an operation to repair esophageal atresia. The first victim of suspected LVNC in this family was a nine year old boy with a history of two episodes of unprovoked convulsion and syncope in school. The first attack was in break time with spasm of neck and body, ended uneventfully. The next one was during exercise, with sudden fall but no urinary incontinence, eye deviation or sialorrhea. The electrocardiogram (ECG), electroencephalography and lab tests showed no abnormalities at that time. He died suddenly during playing after a long period of running. The family lost their 16-year old daughter due to sudden death while she was getting back home after a feast. She also had experienced two seizure episodes associated with loss of consciousness, one at the age of 9 during exercise at school and the other at the age of 10 on vacation. Both episodes had ended uneventfully, and brain CT scan with contrast demonstrated no pathologic finding. We thoroughly evaluated the two cases referred to us. The 12-year-old boy had no history of seizure, syncope, easy fatigability, exertional dyspnea or hospitalization. The ECG showed no ventricular arrhythmia and a normal QT interval. On 2D transthorasic echocardiography, the parasternal short axis and four chamber views demonstrated increased left ventricular (LV) wall thickness accompanied by trabeculations and deep recesses that were indicative of LV non-compaction. The ratio of the compacted to non-compacted regions was 2.18. Also, false tendon was seen at this view (Fig. 1). Color Doppler displayed blood entering these recesses. The coronary arteries were normal and no pericardial effusion and intracavitary thrombi were detected. The 7-year-old girl also had no positive history of hospitalization, seizure, easy fatigue. Her ECG was normal, however, her 2D echocardiograms were compatible with the diagnosis of LV non-compcation, based on the diagnostic criteria already reported by Frischknecht et al[2], with increased lateral, inferior and apical wall thickness and deep recesses and trabeculations. The systolic and diastolic LV functions were normal (FS=38%, LVEF=68%). Color Doppler displayed the blood entering these recesses. The coronary arteries were normal and no pericardial effusion and intracavitary thrombi were detected (Fig. 2). The parents were evaluated clinically and by echocardiography. The findings were normal. Discussion This case report highlights the importance of syncope and seizure as heralding signs for sudden death in two deceased children of a family with two offspring having documented LV non-compaction. Although syncope and sudden death have been previously reported in adults with LVNC but to date, as to best of our knowledge, sudden death with prior heralding sign of syncope and seizure has not been reported in children with LV non-compaction[3]. In our reported family, both of the unexpected deaths occurred after previous episodes of uneventful seizure and syncope. Considering the common embryologic origins of central nervous system and myocardium, occurrence of syncope and seizure in LVNC could be explained[4]. LV non-compaction or persistence of spongy myocardium, first described in 1984[5], is a rare form congenital cardiomyopathy with a prevalence of 0.05-0.24/year. Autosomal dominant and x-linked genetic patterns have been reported. We did not study the genetic pattern in this family[6]. LVNC usually presents with cardiac failure, thromboembolic events, arrhythmia and sudden death[7]. This unclassified cardiomyopathy may be misdiagnosed as hypertrophic or dilated cardiomyopthy[8]. The limitation of our report is lack of echocardiographic evidence for confirmation of diagnosis in the two deceased and not timely-referred and timely-diagnosed children. We suggest careful biannual follow up (ECG, Holter monitoring, Echocardiography) and anticoagulation therapy (Aspirin, dose: 3-5mg/kg/daily) for alive sibling. Conclusion Unexplained seizure and syncope in a child, particularly in a familial pattern, may warrant further echocardiographic evaluation for early diagnosis of left ventricular non-compaction to prevent catastrophic events. Seizure and syncope may be the first manifestations of LVNC. Although the numbers of our patients are limited, but it seems that seizure and syncope can be considered as warning signs in those patients with LVNC who are at high risk for sudden death. References
Copyright 2010 - Iran Journal of Pediatrics |

{kind=link}
{kind=link}