 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
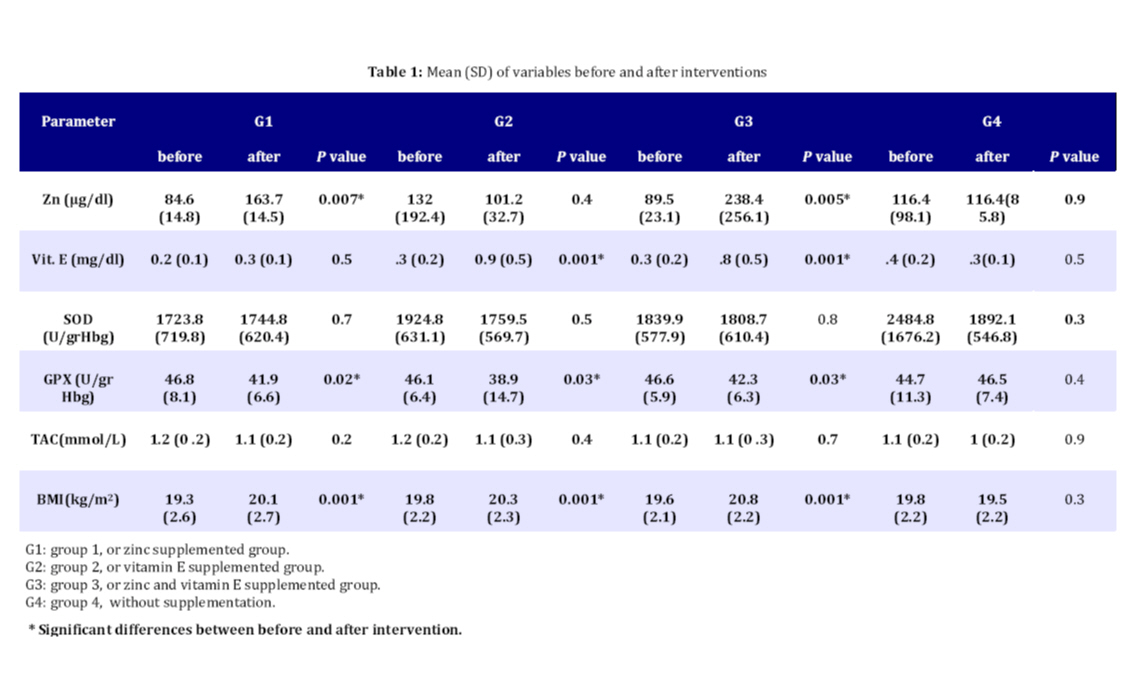
Iranian Journal of Pediatrics, Vol. 20, No. 1, January-March, 2011, pp. 8-14 Effects of Vitamin E and Zinc Supplementation on Antioxidants in Beta Thalassemia Major Patients Mohammadreza Rashidi1, PhD; Maryam Aboomardani2, MD; Maryam Rafraf*3, PhD; Seyed-Rafie Arefhosseini2, PhD; Abbasali Keshtkar4, PhD, and Hamidreza Joshaghani4, PhD
* Corresponding Author; Address: Nutritional Research Center, Faculty of Health and Nutrition, Tabriz University of Medical Sciences, Tabriz, Iran, Email: rafrafm@tbzmed.ac.ir Received: Dec 22, 2008; Final Revision: May 18, 2009; Accepted: Jul 06, 2009 Code Number: pe11002 Abstract Objective: In
beta thalassemic patients, tissue damage occurs due to oxidative
stress and it happens because of the accumulation of iron in the
body. This study was conducted to determine the effect of zinc
and vitamin E supplementation on antioxidant status in beta-thalassemic
major patients. Key Words: Vitamin E; Zinc; Glutathione Peroxidase; Superoxide Dismutase; Body Mass Index; Antioxidants Introduction Beta-thalassemia major results from acute reduction or lack of synthesis of beta globin chains and can be produced by gene mutations. This causes much of the production of alpha-globin chains which are not able to produce hemoglobin tetramer[1]. Nearly 200 million people in the world are affected by thalassemia syndromes[2]. The prevalence of thalassemia gene in the world is about 3%. About 15,000 people are known as thalassemic in Iran, and about 3,000,000 people are carrying thalassemia gene[3]. In beta thalassemia major, tissue damage occurs due to oxidative stress, and it happens because of the accumulation of iron in the body. Spontaneous oxidation of unpaired alpha-globin chains leads to production of super oxide ions and hydrogen peroxide[4-7]. Reduction in the Total Peroxyl Radical Trapping Capacity (TRAP), which indicates decreased antioxidant defense mechanism, is seen in this disease. Toxic oxygen metabolites are scavenged by antioxidant enzymes such as super oxide dismutase (SOD) and glutathione peroxidase (GPX). SOD reacts directly with H2O2 and then enzymes (Catalase and GPX) come to practice. Thus, these three enzymes, in addition to specific roles, work together against oxidant factors[5,8,9]. Vitamin E is the most important fat soluble antioxidant and considered as the primary step for antioxidant defense system. Numerous studies have demonstrated reduced serum level of this vitamin in beta-thalassemic patients[10-12]. One study conducted on beta-thalassemia intermedia patients indicated that vitamin E supplementation improved balance of the antioxidant system and inhibited the process of lipid peroxidation in patients[10]. In addition to vitamin E, zinc deficiencies in beta- thalassemia major patients have been reported in some studies[11,13-20]. Zinc plays several profoundly and biologically important roles such as causing structural effects in more than 300 metalloenzymes like super oxide dismutase. It also plays different antioxidant roles in the body[21,22]. Specific dietary recommendations for thalassemic patients minimize consumption of iron in the diet, and unfortunately result in the reduction of zinc intake[23]. Furthermore, chelator factors administered to prevent the accumulation of iron, cause an excretion effect on zinc in these patients[7,24,25]. Micronutrient deficiencies, especially of vitamin E and zinc in beta-thalassemia major patients have been reported frequently. However, there is no published data about supplementation of these nutrients in thalassemia major patients. So, we conducted a trial to investigate the joint and separate effects of vitamin E and zinc supplementation on antioxidant status such as GPX, SOD and total antioxidant capacity [TAC] in beta thalassemia major patients. Subjects and Methods This double blind randomized clinical trial was carried out on 120 beta-thalassemic major patients older than 18 years admitted to Taleghani and Amiralmomenin hospitals in the Golestan province (northern Iran) in 2009. All patients were characterized for having beta globin gene mutation. Inclusion criteria were the history of continuous treatment with blood transfusion and Desferal as a chelator agent. Exclusion criteria were diabetes mellitus, smoking, hepatitis B and C and consumption of any supplements at least three months before the study. The patients were randomly assigned into four groups including 30 subjects in each group using a random allocation method (random allocation method was a random permuted block or block balanced randomization using 8 characters blocks containing A, B, C and D). The first and second groups were asked to take a supplement of 220 mg zinc sulfate containing 50 mg zinc daily for three months and 400 mg vitamin E supplement daily for three months. The third group took both supplements in similar doses. The fourth (control) group received no supplement. Information about the demographic characteristics was obtained by questionnaire. Weight and height of subjects were measured. The body mass index (BMI) was calculated as weight [kg]/height [m]. Blood samples were obtained from subjects after a 12-hour fasting, just before they received transfusion at beginning and end of the study, and stored at -70 C until assay. Vitamin E and zinc therapy in thalassemic patients started immediately after the first transfusion. Serum vitamin E level was measured by HPLC (Knuer Germany)[7]. In order to determine serum zinc concentration, the samples were collected in trace metal-free tubes to avoid contamination. Serum zinc was analyzed by flame atomic absorption spectrophotometry (Chem’s tech analytical UK, 2000-A.A.S)[26]. In order to assess the enzyme activity of SOD and GPX, the whole blood was rinsed three times with 0.9% saline normal. Activities of GPX and SOD of RBC were assessed by RANCEL and RANSOL (RANDOX, UK) kits. TAC was assessed by TAC (RANDOX, UK) kits. The ethical committee of Tabriz University of Medical Sciences approved the study protocol. Written informed consent was obtained from all patients. Statistical analysis was carried out on Statistical Package for Social Sciences (SPSS for Windows, release 11.0, 2002, SPSS, Chicago, IL, USA). Data were presented as mean±SD. Paired t-test was used for comparison of the mean for changes of different variables before and after intervention phases. Significant level was set 0.05 and all the statistical tests were carried out as two sided. Findings One hundred and twenty subjects including 57 males and 63 females participated in this study. The mean (±SD) age for all groups was 21.1 (±9.7) years. Males' mean±SD age was 21.6 ± 3.8 and for females it was 22.2 ± 4.6 years. Serum zinc concentration in group 1 and 3, was significantly increased (P<0.007 and P<0.005, respectively). Serum concentration of vitamin E, in group 2 and 3 was significantly increased (P<0.001). Mean GPX activity in groups 1, 2, and 3 showed significant decrease (P<0.015, P<0.032 and P<0.029, respectively). Mean BMI in groups 1, 2, and 3 revealed significantly positive changes (P<0.001). Mean SOD activity and serum TAC did not show significant changes in any of the studied groups. No significant difference was seen in fourth (control) group, which did not use any supplements (Table 1). Discussion Red blood cells in thalassemics have morphologic abnormalities, which result in increased susceptibility of thalassemic red cells to the exogenous peroxidant threat. Two mechanisms for inadequate peroxidant defense in thalassemics are insufficient vitamin E levels in red blood cells and plasma, and decreased activity of several enzymes including SOD and GPX, which are the first line of defense against oxidant stress[7]. According to the results (Table1), mean serum levels of vitamin E in all groups at beginning of the study were lower than the normal range[27]. Vitamin E deficiency in thalassaemias is attributed to its increased consumption pursuant to the oxidative stress[5,7]; Chronic hepatic iron overloads, while causing a substantial reduction of serum lipids, can also lead to concurrent reduction of serum vitamin E[28]. Some studies have reported a serum zinc deficiency in beta thalassemia patients, which was related to hyperzincuria resulted from the release of Zn from hemolyzed red cells[18,19,20]. In our studied subjects, 16% had a serum zinc deficiency (data are not shown); however, mean serum zinc was not low. Similarly, Mehdizadeh et al also did not report a zinc deficiency in beta thalassemic patients[29]. Absence of predominant zinc deficiency in our patients may have resulted from regular transfusion therapy. Our findings indicate that supplementation with Zn, vitamin E or both of these causes a significant increase in serum level of zinc in the first group, increased serum vitamin E in the second group, and increased serum zinc and vitamin E levels in the third group with no significant difference in the control group. Therefore, these interventions, especially vitamin E supplementation had favorable effects on serum vitamin E levels in patients, considering that base level of vitamin E in serum of all studied groups was lower than the normal limit. Oxidative stress is the result of an imbalance between free radical production and reduced degradation[30]. An increased oxidant stress and a decreased antioxidant status promote peroxidative damage to cell and organelle membranes. It is well documented that disturbances of oxidant-antioxidant balance occur in hemoglobinopathies, especially in thalassemia and sickle cell diseases[31]. Removal of toxic oxygen metabolites is the putative function of antioxidant enzymes such as SOD and GPX. It has already been demonstrated that oxidative stress induces antioxidative enzymes, including SOD and GPX[5]. Our findings confirm this. As indicated in Table 1, prior to interventions, SOD and GPX activities in all groups were much higher than in those of healthy subjects[31,32]. Significant increase in catalytic activities of SOD and GPX also were found in beta-thalassemic erythrocytes of beta-thalassemic carriers in the study of Filiz et al[31]. The increased activity of SOD in beta thalassemia may be involved in scavenging the superoxide radical (O2-), thereby producing more hydrogen peroxide in the erythrocytes. The increased activity of GPX in beta-thalassemia may be involved in detoxifying hydroxyl radical (OH-). This finding suggests that high iron produces an oxidative stress in cells, which respond by increasing their antioxidant defenses. The increase of intracellular antioxidant enzymes might be hypothesized to be a direct effect of increased intracellular iron on gene expression[5]. Based on our results (Table 1), SOD and GPX activities in subjects were also higher than normal limits at the end of the study. However, GPX activity showed a significant reduction in all treated groups. Therefore, all three types of interventions had protective effects on this enzyme, and were effective in elevating the antioxidant status. These findings confirm the results of other studies[31,32]. Pfeifer et al reported that after vitamin E administration, thalassemic patients presented a significant reduction in levels of erythrocyte RBC-reactive oxygen species (ROS) and serum thiobarbituric acid reactive substances (TBARS), and concluded that it could be useful for reducing oxidative damage in other target organs of beta-thalassemia intermediate patients[33]. Mei-ling Cheng et al demonstrated that supplementation with vitamin E prevents oxidative damage to low-density-lipoprotein (LDL) and erythrocytes in beta thalassemia patients[34]. In addition to vitamin E, it was established that zinc can reduce the iron-mediated oxidation of lipids (including red blood cells), proteins, and DNA[35]. The precise antioxidant role of zinc is unclear, but two mechanisms were proposed; first the competitive effect of zinc with iron and copper on the surface of cell membrane for special protein binding which is specific for preventing the production of the toxic OH radical. The second one is binding to the -SH groups in some proteins and preventing them from oxidation[36]. Sidhu et al found that in zinc and protein deficient rat the activities of GPX, catalase, and peroxidation of lipids were increased[37]. Our results confirmed antioxidant effect of zinc (Table 1), as seen in zinc supplemented group GPX activity also reduced significantly. According to the results (Table 1) SOD activity in groups did not change significantly after supplementation. The study of Rahul Naithani, et al in beta-thalassemia major patients showed that SOD increases significantly, and it may be a compensatory mechanism to keep formation of superoxide anions checked to combat the oxidative stress[32]. Kessab-Chekir, et al observed that iron, ferritin, SOD, GPX and TBARS were increased in 56 beta-thalassemic patients; however, vitamin E and TRAP reduced considerably[5]. Meral, et al reported that because of increased lipid peroxidation in beta thalassemic patients a compensatory increase will be seen in SOD and GPX activity[38]. Our findings confirmed the results of above mentioned study, and showed higher SOD activities in patients. Similar to our findings, Carpino et al indicated despite the increased activity of SOD in transfusion dependent thalassemics, TAC did not change[39]. Dissayabutra et al reported despite vitamin E and vitamin C supplementation in beta-thalassemia major patients, TAC did not change during the study period[40]. It was suggested that various methods, including TAC, developed to measure the total antioxidant capacity of serum, have been indicated as useful tools to predict the risk of free radical-induced tissue damage. Nevertheless, with thalassaemia patients, such an approach appears unsuitable. Changes in contributors such as uric acid and bilirubin, the levels of which increase in thalassaemia because of hemolysis, may mask marked changes in other essential antioxidants[28]. It seems that these conditions also contributed to unchanged SOD activity and TAC in our subjects. Low BMI in beta-thalassemic patients is common[41]. According to findings (Table 1) BMI of all treated subjects increased significantly, which was indicative of well-being of patients and positive effect of supplementation. Similar results were seen in Das et al study[12]. It should be noticed that, we did not evaluate other components of the cellular antioxidant defense system such as catalase, glutathione, uric acid, bilirubin, vitamin C, etc. If more enzymatic and non enzymatic antioxidants were measured, we could have a complete evaluation of the antioxidant status in these patients. So, they are considered as limitations of our study. Conclusion Our findings indicated that beta-thalassemic patients were under enhanced oxidative stress condition, and vitamin E deficiency. Administration of selective antioxidants revealed helpful effects, especially on serum vitamin E and GPX activity as components of antioxidant system, and on general well-being of the subjects. Further studies are suggested with different dose and duration of antioxidant supplements to determine their benefits in beta thalassemic patients. Acknowledgment We thank the Vice- Chancellor for Research Office in Tabriz University of Medical Sciences, Drug Applied Research Center of Tabriz University of Medical Sciences, and Nutritional Research center of Tabriz University of Medical Sciences, for financial supports. Our special thanks to Dr Narges-Belgom Mirbehbahani and Seyed –Jamal Ghaemmagami. The authors also thank the stuffs of Thalassaemia Section of Gorgan Taleghani hospital for their collaboration in sampling as well as beta thalassaemia patients who participated in the study. The registration ID of this study in Iranian Registry of Clinical Trials was# IRCT138811033139N1. Conflict of Interest: None References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11002t1.jpg] |
| |||||||||

{kind=link}