 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 1, January-March, 2011, pp. 33-38 Prevalence of Celiac Disease in Iranian Children with Recurrent Abdominal Pain Referred to a Pediatric Referral Center Fatemeh Farahmand1,2, MD; Vajiheh Modaresi2,3, MD; Mehri Najafi1,2, MD; Ahmad Khodadad1,2, MD; Farzaneh Moetamed1,2, MD, and Zalfa Modarres4, MD
Received: Apr 21, 2010; Final Revision: Aug 02, 2010; Accepted: Aug 20, 2010 Code Number: pe11006 Abstract Objective: Clinical
features of Iranian children with celiac disease (CD) are still unknown
and there is scant information about atypical presentation of celiac
disease from Iran. The aim of this study was to determine prevalence
of CD in Iranian children presenting with functional abdominal pain
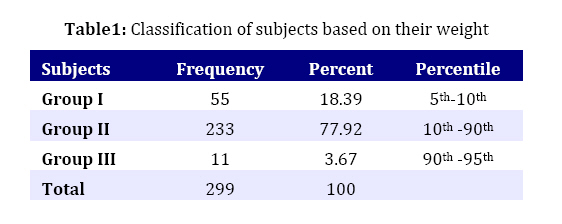
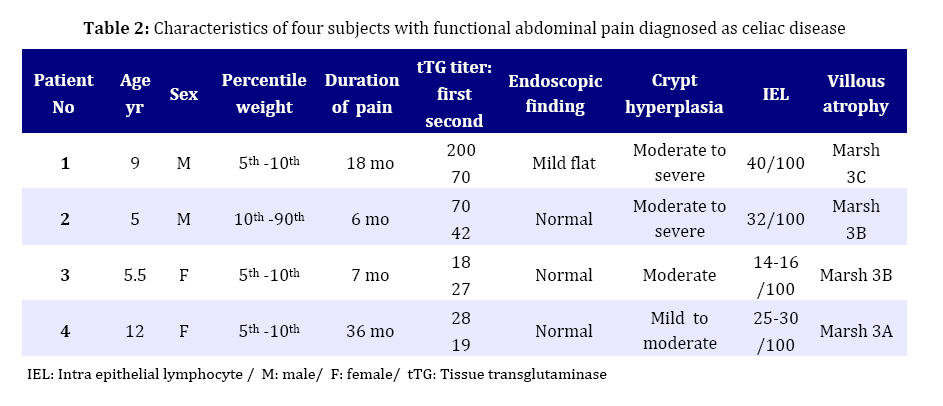
(FAP). Key Words: Celiac Disease; Abdominal Pain; Prevalence; IgA; Malabsorption Introduction Celiac disease (CD), which is induced by ingestion of wheat, rye, and barley proteins, is a chronic autoimmune-mediated disease with both intestinal and extra intestinal manifestations. Some patients present as young children with classical CD and severe malabsorption leading to diarrhea, abdominal distention, growth failure and general malaise[1]. Others develop only mild enteral symptoms or remain asymptomatic for a long time despite having severe small intestinal lesions[2]. The cause of various forms of clinical manifestation in CD is still poorly understood. CD was previously considered to be rare with estimated rate of 0.03% worldwide[1]. However, recently serological screening in healthy volunteers around the world has estimated the prevalence of celiac disease about 0.5-1%[3-5]. Prevalence of celiac disease is also shown to be as high as 1/166 (0.6%) among healthy blood donors in Iran[6]. Active case finding of celiac disease with the use of serum anti-tissue transglutaminase immunoglobulin A (IgA) antibody, usually focuses on patients with typical gastrointestinal symptoms, or known atypical or extra intestinal manifestations, association of which with celiac disease is proven such as isolated iron deficiency, short stature and autoimmune disease or in the first–degree relatives of affected patients[7]. Among the various atypical manifestations of CD, chronic recurrent abdominal pain seems to be an early gastrointestinal manifestation. Chronic abdominal pain is a common childhood experience with reported prevalence of 1-19% and accounting for 2-4% of pediatric office visits, which is a presenting feature of many diseases[8]. In recent studies, celiac disease was considered to be an important cause of chronic abdominal pain in otherwise healthy children; however, it is likely underdiagnosed because of the low index of suspicion. Therefore, we designed this study to determine the prevalence of celiac disease in children with recurrent abdominal pain. Subjects and Methods In this prospective cross-sectional study, we evaluated 301 children with functional abdominal pain (age range 4-15 years) referred to the pediatric gastroenterology clinic of Children's Medical Center in Tehran, Iran. Sample size was calculated based on estimated frequency of celiac disease in children with abdominal pain in a previous study (d=2%). According to Rome III criteria, functional abdominal pain was defined as episodic or continuous abdominal pain without a known underlying organic etiology that occurred at least once per week for at least 2 months before diagnosis [9]. Children with involuntary weight loss, growth retardation, delayed puberty, significant diarrhea or vomiting, gastrointestinal blood loss, unexplained fever, rash, arthritis or a family history of inflammatory bowel or celiac disease, localized tenderness in the right upper or lower quadrant, localized fullness or mass effect, hepatomegaly, splenomegaly, spine or costovertebral angle tenderness, oral ulcer and perianal fissure or fistula, were excluded from the study. We also excluded all the subjects with special risk of celiac disease including positive family history of celiac disease, IgA deficiency, diabetes mellitus, autoimmune disorders, hypothyroidism and Down syndrome from this study. Based on their weight, we classified our subjects into 3 groups that are shown in Table1. Concentrations of serum IgA and anti-tissue transglutaminase IgA antibodies were measured in all patients by the same laboratory using a commercial type of ELISA (Orgentec) test kit. Concentrations of serum IgA and anti-tissue transglutaminase (tTG) IgA antibodies were measured in all patients by the same laboratory using a commercial type of ELISA (Orgentec) test kit. Results were interpreted as follows: negative <16 U/ml, borderline 16-23 U/ml, and positive ≥24 U/ml. The test was repeated for patients with borderline and positive ranges of tTG; and all of them underwent upper gastrointestinal endoscopy (Gastroscope Olympus P230), with at least 4 biopsies taken from the proximal part of the duodenum. The biopsies were interpreted according to the modified Marsh classification by an experienced histopathologist who was blinded to serologic results [10]. The results are reported as mean (±SD). Statistical analysis was performed with SPSS computer package V17 using independent sample t-test, and Mann-Whitney test. P value of less than 0.05 was considered significant. The study protocol was approved by the Research Ethics Board of the Children´s Medical Center, Tehran University of Medical Sciences. All children’s parents gave their written informed consent. Findings A total of 301 children, including 163 (54.2%) females and 138 (45.8%) males were recruited for the study. Mean age of subjects was 7.18±2.71 years and age range 4-15 years. Classification based on subjects' weight is shown in Table 1. Duration of abdominal pain was 10.34±8.12 (range 2-48) months. IgA titer was checked in all of them and only two (0.66%) that had undetectable titer of IgA were excluded from the study. Of the remaining 299 samples that were tested for tTG IgA, 1 patient had intermediate and 3 had high levels of antibody. The test was rechecked in all subjects who had abnormal tTG IgA at the first testing. All these 4 patients underwent upper gastrointestinal endoscopic evaluation and duodenal biopsy. According to histological feature, celiac disease was suspected in all patients with abnormal tTG (Table 2). Discussion This cross sectional study, conducted in the gastroenterology care setting, revealed a frequency of CD in 4/299 of our subjects, that is higher (about two folds) than that found in Iranian general population. The difference in the frequency of CD between children with chronic functional abdominal pain and normal Iranian population was not statistically significant (P>0.05). These findings highlight that in children with chronic abdominal pain, in whom clinical manifestation and history do not fulfill the criteria for special organic disease (known as functional abdominal pain), diagnosis of CD may be missed or delayed. Chronic recurrent abdominal pain in children is still a symptom often difficult to understand and management of patients is frequently disappointing both for family and pediatrician. Actually, finding a definite diagnosis even for a small group of these patients would be an important progress. Although recent studies[11-13] continue to show that non organic pathology can be found to account for the recurrent abdominal pain in the majority of children with no organic cause in 70% of cases as reported by Shahraki in her published study[14]. It should be mentioned that missing a treatable condition such as celiac disease can put the child in serious problems which could easily be prevented by gluten free diet. Comparing the study conducted on normal population in Iran[6], prevalence of CD among children with recurrent functional abdominal pain is nearly two times more than in normal population which is not statistically meaningful (0.6% vs 1.33%). In the last 3 decades, it has become increasingly apparent that CD has been persistently underdiagnosed[15] and that the clinical features of this disease have evolved[16]. Probably less than 10% of those affected present with typical form of celiac disease [17]. Since clinical presentation of CD has changed over time, many affected individuals being asymptomatic are identified only by targeted screening [18]. The classical feature of diarrhea, weight loss, and weakness has been overcome by patients presenting with subtle clinical abnormalities so that initially one would not suggest the diagnosis of this disease. Thus, milder forms such as indigestion, flatulence, or recurrent abdominal pain have become more frequent. With the advent of highly sensitive serological markers, several epidemiological studies have shown that the prevalence of CD in normal population is in the range of 1%[19]. However, association of celiac disease with short stature and diabetes in children in our country, revealed prevalence of biopsy proven CD in 33.6% of children with short stature[20] and in 6.2% of diabetic children[21]. In adults 14.6% of patients with iron deficiency and obscure anemia had CD[22]. Another study from Iran showed that 11.4% of adults whose initial evaluation had led to diagnosis of irritable bowel syndrome, were diagnosed as CD in further evaluation[23]. In this prospective study, we found CD as the cause of FAP of obscure origin in 1.3% of patients. Various rates of prevalence of CD in children with FAP have been reported in different studies[24-26]. A study from Finland reported the prevalence of definite CD among 10-year-old Finish school children 1.2% (at least five out of 404)[26]. This figure is in agreement with 1.33% that is higher compared with normal Iranian population (0.6%) but not statistically significant. As the results of study form India, atypical CD is not uncommon in Iran [19, 27]. Fitzpatrick[24] and Saltik[25] suggested that, according to their findings, CD evaluation is not a necessary test for children suffering from functional abdominal pain.However prevalence of CD was relatively high (1.33%) in our subjects. It seems that the prevalence of CD is as high as to be considered in view of medical interpretation in group of people who are known healthy. Further studies using larger numbers of patients are needed to determine abdominal pain as a sole manifestation of celiac disease in children. It is of interest that our subjects, in whom CD was diagnosed, showed only mild symptoms of abdominal pain but had changes in the small intestinal biopsy specimen compatible with CD. It means that, variable degrees of damage in intestinal mucosa are not correlated with severity of symptoms. Our study also showed that weights of 3 of 4 (75%) CD patients were in the range of 5th-10th percentile according to their sex and age. It seems that CD disease should be particularly considered in children with recurrent abdominal pain whose weight is in low growth curve for sex and age, even in the absence of typical gastrointestinal symptoms. There were some limiting factors to consider in interpreting the study’s result. First, this cross sectional study was conducted on referred children with functional abdominal pain. Ideally, a larger and more popular sample size would perhaps delineate more suitable differences between healthy children and group of children with abdominal pain. Second, this study compared children with normal adult popu-lation, although this would not be statically a problem. As further study, determining true prevalence of disease among normal children could be more helpful. Conclusion In conclusion, this first study determined CD prevalence in children with recurrent abdominal pain and showed that 1.33% of patients with recurrent abdominal pain suffer from celiac disease. Although prevalence of CD in this study was not significantly different (P-value >0.05) from the prevalence rate in healthy blood donors in Iran[6], we think the prevalence is high enough to be considered and recommend to test all children with chronic recurrent functional abdominal pain for CD. Nonetheless, not checking this entity would lead to missing an important problem which could be prevented by a simple change in regular diet. Acknowledgment We are grateful to Dr Fatemeh Mahjob for her precise histology report and Dr Rezaee for editorial assistance. We also thank Dr V. Ziaee for his helpful suggestions. Conflict of Interest: None References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11006t2.jpg] [pe11006t1.jpg] |
| |||||||||

{kind=link}
{kind=link}