 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 1, January-March, 2011, pp. 72-76 Can We Rely on Frozen Sections of a Rectal Biopsy for One-stage Trans-anal Pull-through Operation in Hirschsprung's Disease? Mohsen Rouzrokh*, MD; Farzaneh Jadali, MD; Atoosa Gharib, MD; Ahmad Khaleghnejad Tabari, MD; Azita Tavassoli, MD, and Leily Mohajerzadeh, MD Pediatric Surgery Research Center, Shaheed Beheshti University of Medical Sciences, Tehran, Iran * Corresponding Author; Address: Mofid Children's Hospital, Shariati Ave, Tehran, Iran E-mail: mohsen_rouzrokh@yahoo.com Received: Feb 20, 2010; Final Revision: Aug 10, 2010; Accepted: Sep 17, 2009 Code Number: pe11012 Abstract Objective: Successful
results after one-stage trans-anal pull-through (OSTAPT) operation
for Hirschsprung's disease (HD) depend on accurate identification of
the aganglionic segment in intra-operative frozen section (FS). Misinterpretation
of the findings of the rectal biopsy is an anxiety-evoking pitfall
for the surgeon. This study aims to describe our experiences in comparing
results of FS and permanent Section (PS) rectal biopsies in children
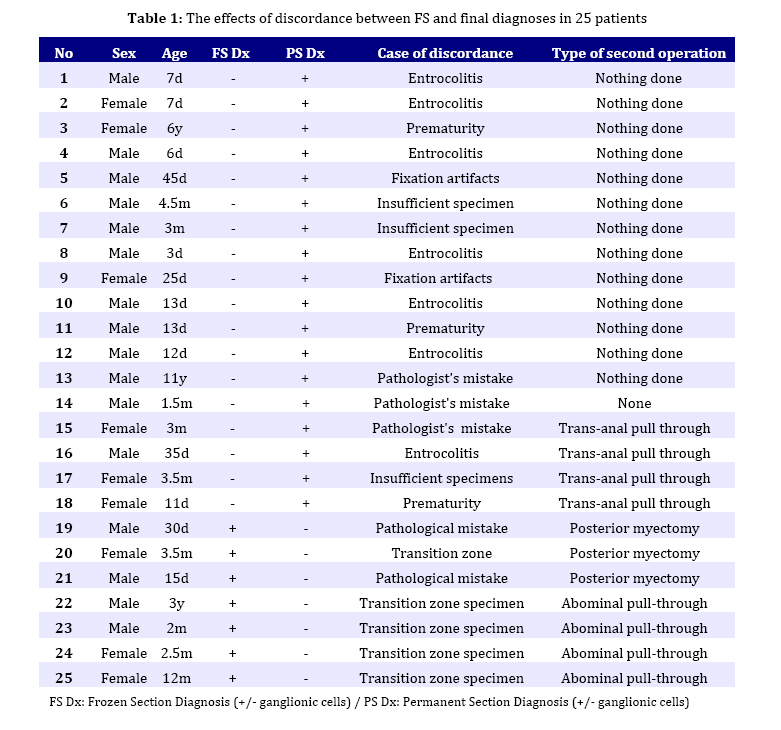
with HD who were candidates for OSTAPT in a single-step operation. Key Words: Hirschsprung's disease; Frozen Section; Rectum; Biopsy; Aganglionic Megacolon Introduction Hirschsprung's disease (HD) is a congenital disorder characterized by absence of ganglionic cells in the large bowel (80-85% in rectosigmoid junction) leading to functional obstruction and colonic dilatation proximal to the affected segment. HD is strongly suspected by presenting symptoms, the radiological appearance of the bowel, and by rectal manometry, but absence of ganglion cells in rectal biopsy is considered as the gold standard for the definitive diagnosis of HD[1] . The traditional diagnostic approach is a full thickness segment biopsy. But alternatives such as suction rectal biopsy are frequently used. Although the rapid acetylcholine esterase staining method has been used for diagnosing HD with good results[2,3,4], it unfortunately was not available in our hospital. Suction rectal biopsy has a high diagnostic accuracy and can be performed at bedside[5]. The most common problem in this technique is an inadequate specimen with an insufficient amount of submucosal neural plexus, so that an evaluation of ganglion cells is precluded. Is biopsy done too close to the anal sphincter and normal hypoganglionic level, the diagnosis of HD will be considerably more difficult than that of a full-thickness biopsy[6,7].. Typical histological feature of HD includes absence of ganglionic cells plus increased number of hypertrophic nerves. These cells are better recognized in Auerbach plexus in full-thickness rectal or colonic biopsies[2]. Full thickness biopsy can be prepared as a frozen section (FS) to be examined promptly, or as a permanent section (PS), which would take about 48 hours before the results become available. In this study we aimed to define the diagnostic accuracy of FS and its concordance with PS in the rectal biopsies of children hospitalized with suspected HD. We intended to find out if we could go ahead with the one-stage trans-anal pull-through (OSTAPT) operation solely on the basis of the histological findings in full thickness FS rectal biopsy. Subjects and Methods From March 2000 to July 2008, all patients (210 cases) with clinical and paraclinical findings highly suspicious of HD were candidates for FS rectal biopsy in Mofid Children's Hospital. Patients with total aganglionic colon on contrast enema were excluded. Two hundred and ten full thickness rectal biopsies (2-3cm above dentate line) were taken from 210 patients. Specimens were obtained for both FS and PS biopsies from all patients. Using cryostat machine, the specimens were prepared at about 3μm thickness and stained by routine hematoxylin and eosin (H&E) staining. Both frozen and permanent sections were examined by two well experienced pediatric pathologists for ascertaining the presence of ganglion cells. Pathological reports with hypoganglionic or neural intestinal dysplasia were excluded and finally 201 full-thickness rectal biopsies evaluated. The accuracy, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated. The concordance between FS diagnosis and PS diagnosis and the causal factors which led to misdiagnosis were identified. To compare the diagnostic accuracy of FS with PS McNamara test was performed. We also report the therapeutic consequences of the actions taken on the basis of results of FS alone. Findings Two hundred and ten patients (151 boys and 69 girls) with mean age of 3.6 months (3 days-14 years) were included in the study. 18.9% of study population were >2 years of age. Nine pathological reports with hypoganglionic or neural intestinal dysplasia were excluded. Comparing the results of FS with PS, findings in 201cases were as follows: In 18 patients, the FS falsely suggested absent ganglion cells, the final PS diagnosis revealed a normal pattern. This group comprises 7 neonates with mild entrocolitis, 3 neonates with prematurity, 3 insufficient specimens, 2 fixation artifacts and 3 specimens with pathologist's misinterpretation. In 4 out of these 18 patients, trans-anal pull-through operation was carried out solely on the basis of FS; however, in the other 14 subjects the surgeon decided to wait for the results of PS, which revealed the presence of normal ganglions, thus avoiding an unnecessary major surgery. Conversely, in 7 cases FS falsely reported normal ganglion cells and accordingly the operation was ended; but PS revealed absence of ganglionic cells. Confounding factors in this group: 5 specimens were taken from the transition zone (in low segment HD) and 2 specimens were not satisfactory for microscopic examination. In 4 of these patients abdominal pull-through operation was done and in 3 children with low segment HD, myectomy was performed (Table 1). 54.7% of FS samples and 63.8% of PS sections were positive for the presence of ganglionic cells. 93.9% of positive results in FS studies were confirmed by PS diagnosis. 6.1 % of FS reports were false positive and 21.7% false negative (P<0.001). The sensitivity of FS was 85.8% and its specificity 90.2%. Positive predictive value (PPV) was 93.9% and negative predictive value (NPV) 78.3% in FS studies (P<0.001). The accuracy of FS biopsy was 80.4%. Discussion The approach to surgical treatment of HD has changed recently. Most of the affected children can be treated with a primary pull-through by several techniques (transanal, trans-abdominal and laparoscopic pull-through)[8,9]. Rectal biopsies make up the cornerstone for the diagnosis of HD and subsequent surgery[8]. Typical histological findings for HD in rectal biopsy include absence of ganglion cells in both the submucosal (Meissner’s) plexus and the intermuscular (Auerbach’s) plexus [3,10]. Rectal biopsy may be obtained by means of suction or full thickness seromuscular method, both techniques having some advantages and disadvantages. The suction biopsy is difficult to interpret than full-thickness biopsy. When the diagnosis cannot be made by suction biopsy of rectum, a full-thickness posterior rectal wall biopsy should be performed[2]. In the surgical treatment of HD, there is a trend towards primary resection without colostomy by transanal or transabdominal approach (open or laparoscopic). This renders significant importance to the evaluation of the initial pathologic specimen[7,10,11]. In patients with strongly suspected HD, open rectal biopsy is taken and after definite diagnosis of HD by FS, definitive surgery is performed as a single-step procedure[9]. Our research showed that in 80.4 % of cases there was complete agreement between the findings of FS and PS among the 201 children with HD. The reported concordance rates between the results of frozen sections and the permanent sections reported by other authors range from 67-100%[6,11,12]. Factors that contribute to errors in FS as reported by other authors include: transitional zone sampling, freezing artifact, recognition of immature ganglion cells, superficial sectioning of the FS biopsy, technical difficulty in FS preparation, inexperienced pathologist, and the appendix sampling[12,13]. In our series, the most common factors that affected FS results were: fixation artifact, insufficient biopsy samples, pathologist's mistake, and also confounding factors such as entrocolitis, short segment aganglionosis, existence of inflammation or scar in a previous biopsy site, premature neonate, and the transition zone biopsy. Conclusion The role of FS in the diagnosis of HD can not be denied, especially in ascertaining the presence of the ganglionic segment during surgery. Although error rate is low with a frozen section, the potentially serious clinical consequences of these errors are significant, such as unnecessary surgery or a second operation. We recommend that the absence of ganglion cells in FS rectal biopsy for possible HD should be established by final PS diagnosis and definitive surgery should only be done if the findings are confirmed by permanent section. Acknowledgment This study was approved by the Ethical Committee of the faculty of medicine of Shahid Beheshti Medical University. The authors would like to thank the director and the staff of the Pediatric infections Research Center of Shahid Beheshti Medical University for their help in preparing the manuscript Conflict of Interest: None References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11012t1.jpg] |
| |||||||||

{kind=link}