 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 1, January-March, 2011, pp. 83-87 Entrobacter, the Most Common Pathogen of Neonatal Septicemia in Rasht, Iran Mohammad-Mehdi Karambin, MD, and Marjaneh Zarkesh, MD Department of Pediatrics, Guilan University of Medical Sciences, Rasht, Iran * Corresponding Author; Address: Department of Pediatrics, School of Medicine, Guilan University of Medical Sciences, Guilan, Iran E-mail: karambin@gums.ac.ir Received: May 25, 2010; Final Revision: Sep 19, 2010; Accepted: Oct 03, 2010 Code Number: pe11014 Abstract Objective: Bacterial
sepsis continues to be a major cause of morbidity and mortality in
newborns. Bacterial pathogens of neonatal septicemia may vary from
one country to another and within a country from one hospital
or region to another. Both gram-negative and gram-positive bacteria
are responsible in neonatal sepsis. This study was undertaken to determine
the prevalent bacterial agents of neonatal sepsis and their antimicrobial
susceptibility in a teaching hospital, Rasht, from February 2008 to
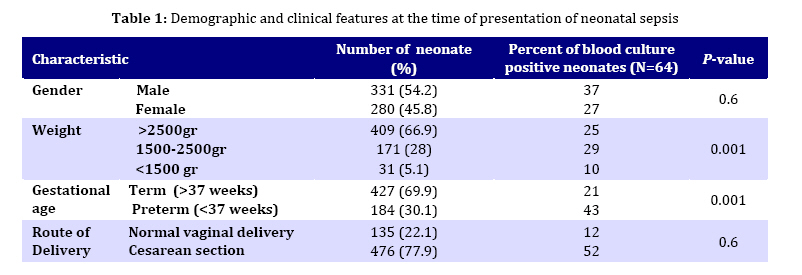
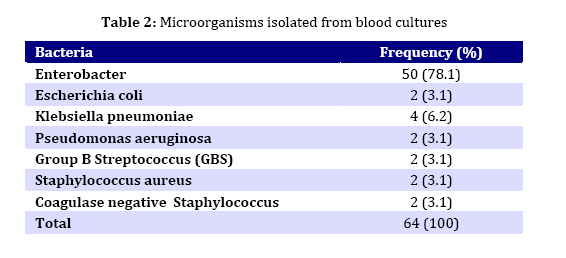
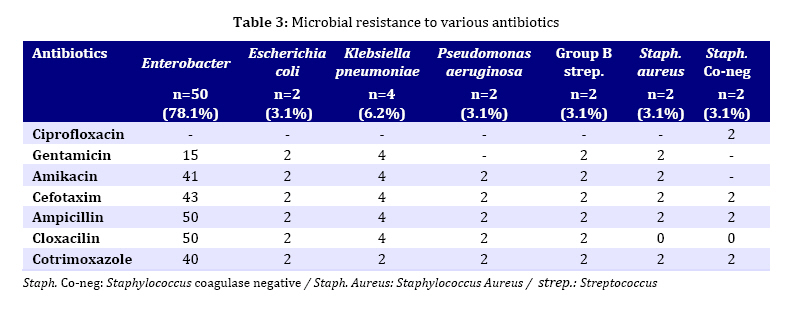
February 2010. Key Words: Neonate; Sepsis; Antibiotics; Drug Resistance; Entrobacter; Bacterial Infection Introduction Sepsis neonatorum is the term used to describe any systemic bacterial infection documented by a positive blood culture in the first month of life[1]. Bacterial pathogens of neonatal septicemia may vary from one country to another and within a country from one hospital or region to another[2]. So regional study is helpful. Neonatal sepsis can be classified into two relatively distinct illnesses, early onset sepsis (EOS) occurs in the first 7 days of life, late onset sepsis (LOS) occurs ≥7 days to 3 months of life[1]. The leading cause of EOS in term infants is Group B streptococus (GBS), and in preterm infants gram-negative enteric bacteria. Nearly half of cases of LOS are caused by coagulase–negative staphylococci (CONS); also other Gram-positive (22%) and Gram-negative organisms (18%) as well as fungal sepsis (12%) can cause LOS[3]. In another classification, Early-onset bacteremia (occurring within 72 hours after birth) is currently caused by predominantly aerobic Gram-positive organisms and late onset is due to predominantly aerobic Gram-negative bac-teria[4]. Early-onset neonatal sepsis is caused by microorganisms acquired from the mother before or during birth (vertically transmitted and perinatally acquired); thus, microorganisms from the maternal genital tract may play an important role in early infection[5]. In late-onset neonatal infections, a low proportion of neonates are infected at the time of birth; others are born prematurely and/or have a very low birth weight[6]. Bacteremia remains a significant cause of morbidity and mortality in neonatal period. In the United States alone, it is estimated that 200,000 cases of bacteremia occur annually, with mortality as high as 50%[7]. In Iran, Gheibi et al[8] showed that the overall sepsis rate of 4.7 percent of all admissions fall within the range quoted in the literature. Of the 2325 neonates screened for sepsis, there were 258 (11%) positive blood cultures[8]. Identification of the etiology is important since it can induce a change in management policy[2], and study of bacteriological profile and their antibiotic sensitivity pattern plays a significant role[4-6]. The present study was carried out to determine the prevalent bacterial agents of neonatal sepsis and their antimicrobial susceptibility in our hospital from February 2008 to February 2010. Subjects and Methods In a prospective study during 2 years, a total of 611 blood samples for culture were obtained from neonates having a clinical picture suggestive of septicemia/bacteremia (poor feeding, respiratory distress, fever, hypothermia, gastrointestinal and/or central nervous system symptoms) who were hospitalized in neonatal ward of 17 Shahrivar Children's Hospital. Two blood cultures, complete blood count (CBC), erythrocyte sedimentation rate (ESR), C‐reactive protein (CRP), blood sugar, electrolytes, cerebrospinal fluid (CSF), chest X-ray (CXR) and urine analysis/culture were tested in all cases of suspected neonatal sepsis. Standard procedure of sample collection and culture was undertaken with aseptic precautions. For blood cultures two samples of 1 ml blood were taken from two different sites, inoculated in trypticase soy agar, incubated at 35‐37°C and examined daily for evidence of bacterial growth. Sensitivity of the bacterial isolates to different antibiotics was determined using standard disc diffusion (SDD) method[9]. When growth appeared, the culture was inoculated into a blood agar plate and a gram‐stained smear was examined. Antibiotic sensitivity was tested for ampicillin, gentamicin, amikacin, cefotaxim, cloxacillin, ciprofloxacin, and co-trimoxazole. Meningitis was diagnosed with positive CSF cultures, pneumonia according to clinical signs and CXR findings and urinary tract infection (UTI) with growth of any pathogen in suprapubic urine sample. The ethics committee of Guilan University approved the study. Low birth weight (LBW) was defined as birth weight <2500 grams and preterm neonate when born before 37th week following onset of the last menstrual period. All statistical analyses were performed using SPSS statistical program (version 16 for Windows). The chi-squared test and Fisher′s exact test were used. P-value <0.05 was considered significant. Findings Among 611 neonates there were 64 (10.4%) positive blood cultures (Table 1). The median age of proven septic cases was 16 days from a range of 2-28 days. 37 (11.2%) of 331 male neonates and 27 (9.6%) of 280 female newborns had positive blood cultures (P-value was not significant). Lower birth weight and prematurity were associated with higher risk of sepsis significantly (P=0.001). Twenty-nine (17%) of 171 neonates with birth weight 1500-2500 grams had at least one episode of blood culture proven sepsis. 10 (32.3%) of 31 cases with birth weight <1500 grams had proven sepsis. the rate of infection decreased with increasing birth weight to 25 (6.1%) of 409 infants with birth weight >2500gr. Similarly, the infection rate was inversely related to gestational age (GA). 43 (23.4%) of 184 neonates who were born <37 weeks of gestation (preterm) developed proven sepsis. This declined to 21 (4.9%) of 427 term newborns (P=0.001). 12 (8.9%) of 135 neonates who were born by normal vaginal delivery (NVD) and 52 (10.9%) of 476 neonates who were born by cesarean section (CS) had proven sepsis (P was not significant). From 64 neonates with positive blood cultures, 5 (23%) neonates had EOS and 49 (77%) LOS. UTI, pneumonia or meningitis was diagnosed in 1, 6 and 0 cases of EOS and 18, 10 and 4 neonates of LOS respectively. From all positive cultures were gram negative bacteria isolated. Enterobacter was detected in 50 patients (16 term and 34 preterm neonates). Other bacterial etiologies included Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa as well as Group B Streptococcus, Staphylococcus aureus, and coagulase negative Staphylococcus. The percentage of isolates from culture positive neonates is shown in Table 2. Enterobacter isolates were frequently found to be resistant to cloxacilin, ampicillin, cefotaxim, amikacin, and co-trimoxazole. Ciprofloxacin was found to be the most effective drug (Antibiotic sensitivity is shown in Table 3). Discussion In the present study, positive blood cultures were obtained in 10.4% of the suspected cases of septicemia, which is in conformity with earlier reports[5]. Since signs and symptoms of sepsis overlap other disorders (such as intraventricular hemorrhage, asphyxia, metabolic disorders), overdiagnosis of septicemia is a common problem. Nevertheless negative cultures do not rule out the possibility of neonatal sepsis and may be due to several reasons, e.g. administration of antibiotics before blood collection either to mother or baby, or the possibility of infection with viruses, fungi or anaerobes, which cannot be ruled out[7]. In developing countries, rates of blood stream infections have been reported to be 1.7 to 33 per 1,000 live births and in Asia clustering around 15 per 1,000 live births[10]. Findings of this study indicate that low birth weight, prematurity and male sex were associated with higher risk of sepsis. The rates of prematurity and low birth weight, both of which predispose to neonatal infection, are inversely related to socioeconomic status. It was noted in 1960s that male infants had a higher incidence of neonatal sepsis than female infants. Possibly this is related to x-linked immunoregulatory genes[1]. The high percentage of newborns born with CS was due to high frequency of elective CS in Rasht. EOS was more associated with pneumonia, LOS with UTI. In the present study, Gram negative organisms constituted the major group of isolates from neonatal septicemia cases. Among this group Enterobacter species has been found to be the predominant pathogen (78.1%) (Table 2). Since etiologic agents in neonatal EOS and sometimes LOS are often acquired from mother's genital tract, vaginal cultures in all pregnant women as a screening program and appropriate treatment of positive cases before delivery should be emphasized. In a study in Tabriz, Ghotaslou et al[11] showed that among 210 cases of neonatal sepsis the most common organism was coagulase-negative staphylococci. Gram-negative organisms were isolated in 66 (31.43%) cases, and the most common Gram-negative organism causing neonatal sepsis was Klebsiella pneumoniae. The mortality rate due to Gram-negative bacteria including K. pneumoniae was higher than that caused by other bacteria. The distribution of the main pathogens is different in Azerbaijan province, northwest Iran, where K. pneumoniae is predominant, and Streptococcus plays a relatively minor role in the etiology of sepsis during the first month of life[11]. Agnihotri et al showed that among 3,064 suspected cases of septicemia, 588 (19.2%) were positive for bacterial isolates. The incidence of Gram-negative and Gram-positive organisms was 58.5% and 41.5%, respectively. There were 379 (64.5%) isolates from early onset (age ≤1 week) septicemia cases, while 209 (35.5%) were from late onset (age >1 week) illness[12]. The predominance of Gram-negative organisms corroborates the finding of other workers[13]. In the United States, gram positive cocci, including group A streptococcus were the most common pathogens before the introduction of antibiotics, but this predominance shifted to Gram negative enteric bacilli after antimicrobial agents came into common use[10]. Neonatal septicemia is a life-threatening emergency, and rapid treatment with antibiotics is essential for a favorable outcome. With the advent of the third-generation cephalosporins, the empiric antimicrobial approach for neonatal sepsis has changed in many centers. The results of antibiotic sensitivity revealed that majority of our bacterial isolates were sensitive to ciprofloxacin and gentamicin. The antimicrobial sensitivity pattern differs in different studies as well as at different times in the same hospital. This is because of emergence of resistant strains as a result of indiscriminate use of antibiotics. In the present study, Enterobacter isolates were frequently found to be resistant several antibiotics thus indicating that the use of these drugs alone may be ineffective (Table 3). These findings are similar to those described by Agnihotri et al[12]. Thus, our study suggests that gentamicin is the most suitable drug for the treatment of neonatal septicemia according to in vitro susceptibility results and should be used in empiric therapy of neonatal sepsis with ampicillin or vancomaycin. Because of side effects of ciprofloxacin, we do not suggest routine use of it in neonatal sepsis. Multiple changes have occurred in recent years with increasing awareness of prevention of sepsis. These changes include: prevention of preterm labor also earlier and more aggressive enteral feeding and the resultant early discontinuation of vascular catheters, shorter duration of invasive ventilation because of surfactant use, better hand hygiene practices and better protocols for handling vascular lines[13]. The limitation of our study was positive history of systemic antibiotic administration in some neonates before admission in our hospital which caused the cultures to be negative and also positive history of admission in other centers before referring to our hospital which might have caused nosocomial infection. Conclusion In the present study, positive blood cultures were obtained in 10.4% of suspected cases of septicemia. Low birth weight and prematurity were associated with higher risk of sepsis significantly. Also positive blood cultures were more common in male neonates. Gram-negative organisms constituted the major group of isolates from septic cases. Among this group Enterobacter species has been found to be predominant pathogen accounting for 78.1% of cases. Our study suggests that gentamicin is the most suitable drug for treatment of neonatal septicemia as per in vitro susceptibility results. Acknowledgment Our thanks go to all who participated actively in this study especially our neonatal ward nurses. Conflict of Interest: None References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11014t2.jpg] [pe11014t1.jpg] [pe11014t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}