 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 1, January-March, 2011, pp. 99-102 Use of “Kangaroo Care”to Alleviate the Intensity of Vaccination Pain in Newborns Reza Saeidi1, MD; Zahra Asnaashari1, MSc; Mohtaram Amirnejad1, MSc; Habibollah Esmaeili2, MSc, and Mahboobe Gholami Robatsangi3, MSc
* Corresponding Author; Address: Midwifery Group Room, Islamic Azad University, Pajoohesh Ave, Neyshabur, Iran E-mail: midwiferymaster26279@gmail.com Received: May 20, 2009; Final Revision: Dec 08, 2009; Accepted: Apr 02, 2010 Code Number: pe11017 Abstract Objective: It
has been demonstrated that newborns feel pain completely. Thus, they
should be treated with this in mind. Recent research showed that
non-pharmacological interventions such as “Kangaroo Care”may
be useful for decreasing pain in newborns. We tried to determine
the effect of kangaroo care on the pain intensity of vaccination
in healthy newborns. Key Words: Kangaroo Mother Care; Pain; Newborn; Vaccination; Infant Care Introduction Pain is a complicated phenomenon often ignored in newborns[1]. Until the last decade of 1970, it was thought that infants cannot feel or recall pain, so surgical procedures in infants were carried out without anesthesia or analgesia[2]. Later, research showed that the fibers that transfer the pain stimuli are organized in the fetus. The nerve pathway myelinization begins in the 2nd and 3rd trimesters and finishes between 30 to 37weeks of gestational age[2]. M Koban et al (2003) also showed that insufficient pain control results in hypoxia and stimuli reaction[3]. Thus, pain relief in infants is important and necessary. Analgesia is achieved with pharmacologic and non-pharmacologic methods[4]. Kazak et al compared effect of pharmacologic and non-pharmacologic treatment on pain and concluded that non-pharmacological methods are more effective than pharmacological methods for pain relief[5]. This has helped the mother-infant bond and increased the mother's self-esteem and skills[6]. Studies have shown that Kangaroo mother care (KMC) is effective on infant pain[7-10]. Kangaroo care originated in Bogotá, Colombia because of a lack of incubators for preterm infants[11]. During KMC the adult holds the diapered infant against his/her skin[11]. The infant lies upright on the adult's chest. A breastfeeding mother may allow the infant self-regulatory access to her breast. The adult is without clothing from the waist up; a blanket covers both the infant and adult[11]. KMC has three provisions: 1) Skin to skin contact, 2) exclusive breastfeeding, 3) support to the mother and infant[12]. Care-giving and analgesia is in the domain of nursing activities and must be a priority in nursing standards. This study sought to assess the effect of KMC on vaccination pain in infants. Subjects and Methods This was a semi-experimental double blind, double group, and clinical trial study approved by the research ethics committee of Mashhad University of Medical Sciences. Sixty infants born during March to July 2006 with the following inclusion criteria: born at term with a weight between 2500 to 4000 g, type of delivery NVD, Apgar score 1=7-10, at earliest 24 hr after birth, not fed since 30 minutes and lack of skin lesions in mother or infant, were studied. Sampling method was nonrandom and proposed. Samples were divided randomly into two groups. In the case group, the mother was requested to put the baby under her gown between her breasts with maximum skin to skin contact. The time of skin to skin contact was 2 minutes before vaccination and 3 minutes afterwards. Pulse rate, O2 saturation and crying time were recorded using a chronometer. Neonatal reactions to pain were video-recorded. The film was watched by an assistant blinded to the research. Behavioral changes were scored according to Neonatal/Infant Pain Scale (NIPS) recommended for children less than 1 year old. In this scoring a score greater than 3 indicates pain.
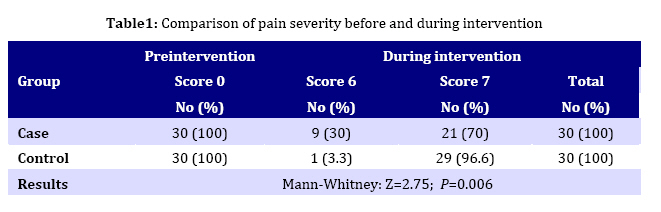
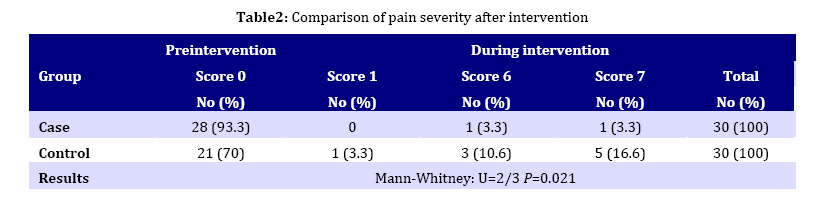
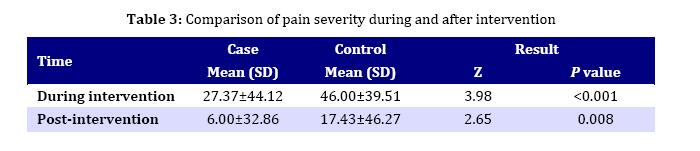
Babies in the control group were wrapped in a blanket and put near the bed of their mothers. We recorded the physiologic and behavioral reactions of these infants to pain using the same method as for the case group. Data were analyzed using Chi-square, Fisher exact test, paired t-test and independent t-test and Mann-Whitney test. Findings The case group consisted of 53% were males and 47% females whereas in controls 60% were females and 40% males; 80% of the case group and 73.3% of the control group had 40 weeks gestational age; 83.3% of the infants in the case group and 96.7% in the control group had a first minute Apgar score of 9. Mean birth weight in the case group was 3242±306.6 and in the control group 3151±331.5 grams. According to the results obtained from the NIPS score, during intervention 30% of the infants had a pain score of 6 and 70% in the case group 7, while 96.6% of the neonates in the control group had a score of 7 and 3.3% had a score of 6. This was statistically significant (P<0.001, Table 1). Three minutes after intervention 93.3% of the infants in the case group had pain score 0 and only 6.6 had 6 to 7 pain scores while in the control group 70% had a zero pain score and more than 26% had a 6 or 7 pain scores. This was also significant (P=0.021, Table 2). Mean pain intensity 3 minutes after intervention was significantly lower in the case than control group(P=0.008, Table 3). According to Mann-Whitney test there was a significant statistical difference in the cry interval times between the 2 groups (P<0.001) during intervention. There was a significant statistical difference between the 2 groups in the time interval of crying after intervention (P=0.008). The preinterventional O2 saturation in the case group was 95.80±2.78 and 94.07±3.18 in the control group, during intervention 96.17±2.61 in the case group and 94.53±2.64 in control group and after intervention 95.60±2.19 in case group and 95.10±1.72 in the control group. O2 saturation was statistically insignificant (P=0.1). Crying interval during intervention and after intervention was statistically not significant (P=0.08). Discussion Mean pain intensity during intervention was significantly lower in the case group than in control group. Mean pain intensity 3 minutes after intervention was significantly lower in the case than control group. Mean duration of crying was significantly lower in case group as well. This was compatible with the results of the Gray et al and Johnston et al[8,13]. Gray et al showed that pain reaction was 65% less in their case group compared to the control group[8]. The results of Johnston et al showed that the efficacy of the KMC was significant in relieving pain in infants of 32 weeks gestational age[13]. The results of Anderson et al showed that skin to skin contact is a factor that relieves infant pain and reduces behavioral and physiological reactions to painful stimulations[9]. Moreover, Luedington investigated the effect of skin to skin contact on painful nursing procedures. He concluded that infants who had skin to skin contact showed less pain related reactions such as change in grimace[10]. Our study was compatible with Johnson’s with regard to pulse rate in the two groups which was insignificant[13]. Gray reported that hugging neonates during vaccination decreased the crying interval compared to the control group in which the neonates were placed on a bed during vaccination[8]. The present investigation showed that the skin to skin contact group had a crying interval time shorter than that of controls. Conclusion According to the results of this study KMC decreased pain severity in neonates of the case group during the intervention and 3 minutes afterwards. Kangaroo care is a useful procedure recom-mended in painful procedures of newborns. Acknowledgment The authors would like to thank Mrs. Z. Ahmadi and the Research Committee of Mashhad University of Medical Sciences for their help. Conflict of Interest: None References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11017t1.jpg] [pe11017t3.jpg] [pe11017t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}