 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 2, Apri l-June, 2011, pp. 166-172 Transcatheter Closure of Atrial Septal Defect with Amplatzer Device in Children and Adolescents: Short and Midterm results; an Iranian Experience Mostafa Behjati*1, MD; Sayed-Jalil Mirhosseini2, MD; Saiyed-Habibollah Hosseini3, MD; Shahrokh Rajaei4, MD
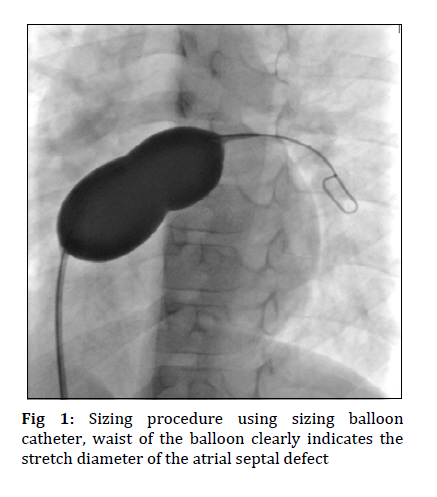
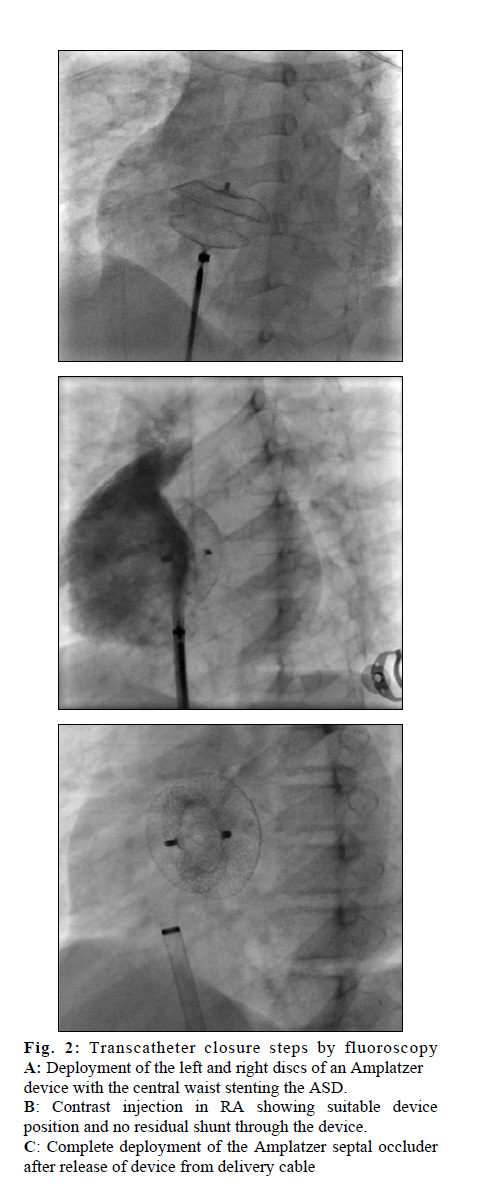
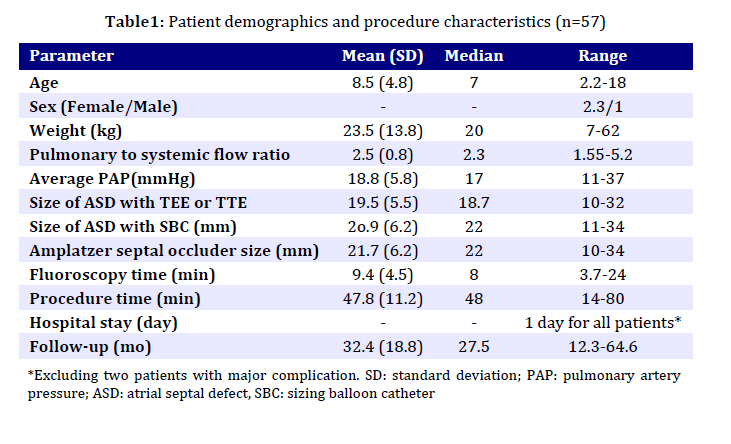
Received: Feb 11, 2010; Final Revision: Nov 06, 2010; Accepted: Dec 26, 2010 Code Number: pe11029 Abstract Objective: Transcatheter closure of secundum atrial septal defect (ASD) with Amplatzer device is an alternative procedure to surgical repair, with some limitations. The aim of this study was to assess the initial and mid-term results of the treatment of ASD with Amplatzer septal occluder in children and adolescents. Key Words: Atrial Septal Defect; Amplatzer;children; Adolescents; Transthoracic Echocardiography Introduction Atrial septal defect (ASD) is common congenital anomaly, accounts for 6% to 10% of congenital heart lesions at birth[1]. It is however one of the most common congenital heart diseases in adulthood[2]. Although the results of surgical repair are good, it is associated with discomfort, morbidity and a thoracotomy scar[3]. Trancatheter intervention in children with congenital heart disease has advanced rapidly in recent years and represents a growing field of invasive pediatric cardiology. A number of devices have been developed for transcatheter closure of ostium secundum type ASD, since first described by King and Mills in 1976[4,5]. Recently, Amplatzer septal occluder (ASO) with unique design and easy handling has finally replaced surgical ASD closure in many centers as the standard treatment for pediatric patient with secundum ASDs[5]. Previous studies have shown high success rate, low complication rate and less discomfort[6,7]. The aim of this study was to evaluate the efficacy and safety of the Amplatzer device over the short and intermediate-term for closure of ASD in children and adolescents. Subjects and Methods From May 2003 to January 2008, a total of 71 patients were referred for transcatheter cardiography of ASD. Seven patients were excluded after initial echocardiographic evaluation: 5 patients with insufficient rim margin, 1 patient with a sinus venous ASD and 1 patient with total anomalous pulmonary venous return. Thus, 63 patients with significant ASD were considered for Inclusion criteria for patients with ASD were: 1) the presence of a secundum ASD with significant left to right shunt (QP/QS ≥1.5/1), 2) ASD with a balloon stretched diameter of 34 mm or less with suitable septal rim of at least 4 mm from the mitral and tricuspid valves, pulmonary veins and coronary sinus, 3) right ventricular overload, 4) patient age 18 years or younger. Exclusion criteria: 1) ASD other than secundum type, 2) abnormal venous drainage, 3) associated complex cardiac anomaly, 4) severe pulmonary hypertension with bi-directional or right to left shunting, 5) a rim of <4mm between defect and cardiac structures. Informed consent was obtained from guardians of all patients. Device: The principle of the device is based on the conjoint waist ''stenting'' the ASD, providing both fixation and occlusion. The ASO is a self-centering and self- extracting occlusion device made from a nitinol wire mesh forming a left atrial retention disc, a self-centering stent and a right atrial disc. The ASO is available in sizes with 1mm increments from 4mm to 20mm and then in 2mm increments until the current largest device of 40 mm. The device is attached to the delivery cable by a central screw at the proximal end of the device. Before introduction the device is collapsed into a tubular loader by pulling on the delivery wire. A 6F to 12F delivery sheath is used depending on the required size of the device[6,7]. Procedure: Before catheterization, transthoracic or thrans-esphageal echocardiography was done with or without sedation to evaluate the size and location of defect and margin. All procedures were performed under local anesthesia and moderate sedation or generalized anesthesia, with transthoracic echo-cardiography, fluoroscopy guidance throughout. First, a standard right heart catheterization was performed through the right femoral vein with recording of blood pressure and blood sampling to calculate the QP:QS ratio. Right upper pulmonary vein angiography in hepatoclavicular view was performed to visualize the atrial septum. For bacterial endocarditis prophylaxis, patients received cefazolin 33 mg/kg (maximum dose 1 g) 30 minutes before the procedure, followed by 33 mg/kg intravenously every 8 hours for an additional 2 doses. After sheath placement, heparin (100units/kg, maximum dose 3000 units) was given intravenously. A sizing balloon catheter (AGA Medical Corporation, Golden Valley, USA) was inflated at the level of defect until the waist in the middle of the balloon was seen (Fig. 1). The waist was measured and calibrated on the Cine-angiographic frame as well as by calibrated template. A device with a waist diameter similar to, or in large defect, up to 2 mm bigger than the stretched ASD diameter was chosen. The selected ASD device was attached to the delivery cable by the screw mechanism and was loaded by withdrawing into the loader by traction on the delivery cable. The collapsed ASO device was then advanced through the long sheath that had previously been positioned in the left atrium. Under fluoroscopic control the left atrial disc was extruded by advancing the delivery cable. The extruded disc, sheath and delivery wire were withdrawn as a single unit until resistance to further withdrawal was met when the extruded left disc was apposed to the atrial septum. The ASO device was then fully deployed by drawing the sheath over the delivery cable to expand the right atrial disc. The position and stability of ASO device was assessed by fluoroscopy and transthoracic echocardio-graphy (TTE). Care was taken to ensure that the device did not obstruct the right pulmonary veins, caval veins, coronary sinus, or the mitral valve. Any residual shunt was evaluated by color Doppler echocardiography on TTE. It was defined as mild (<2mm), moderate (2- 4mm) or severe (>4mm) color jet width. The device was then released from the delivery system and final assessment of the position of the device was performed by TTE. After the release of device, right atrium angiography with follow-through was performed in hepatoclavicular projection (Fig 2). A: Deployment of the left and right discs of an Amplatzer device with the central waist stenting the ASD. B: Contrast injection in RA showing suitable device position and no residual shunt through the device. C: Complete deployment of the Amplatzer septal occluder after release of device from delivery cable Follow-up: In routine, after ASD closure, the patients remained in general ward of the hospital for one night, and received heparin 100 IU/kg/daily (PTT 50-60s) for 24 hours. Transthoracic echocardiography was repeated 24 hours after the procedure and before hospital discharge to ensure suitable deployment of the device. The patients were discharged on ASA (80mg) for 6 months in order to prevent excessive thrombus formation on the device. Standard bacterial endocarditic prophylaxis was recom-mended for 6 months or until complete closure was obtained. A repeat transthoracic echocardiography was performed 1, 6 and 12 months after procedure and yearly thereafter. Data collection and analysis: All data were collected on a set data sheet, collated by a single coordinator, and entered into a common database for analysis. Data expressed as mean standard deviation, median, range and percentage. The data was analyzed using the computer program SPSS version 13.0. Event- free survival was estimated using the Kaplan- meier curve. Outcome measures: Efficacy and safety is defined as follow: Efficacy: The successful closure of defect without residual shunt or only trivial shunt after six months. Safety: The avoidance of death or major complications (cerebral embolism, cardiac tamponade, device embolization or dislodgement requiring open cardiac surgery and infectious endocarditis). Residual shunting following device closure was evaluated by color Doppler transthoracic echocardiography. It was classificated as trivial (<1mm), small (1-2mm), moderate (2-4mm) or severe (>4mm) in diameter of color jet[8]. Findings A total of 63 patients were considered for transcatheter closure with the Amplatzer septal occluder. At catheterization, four further patients were not implanted: in three patients the arterial size was thought to be insufficient to accommodate to occluder size required for defect closure. One patient was excluded because of anomalous right superior pulmonary vein connection to the superior vena cava. Reasons for exclusion included: body weight less than 7kg, severe pulmonary hypertension, and drainage of the right pulmonary veins to the superior vena cava, QP/QS of less than 1.5 and large defect with insufficient margin. Demographic characteristics of the patient and procedure details are summarized in Table 1. The average procedure time and fluoroscopy time were 47.8±11.2 min and 9.4±4.5 min respectively with a tendency to shorter procedural and screening time after the learning curve. Two serious complications were observed: dislodgment of device in 1 and device emboli-zation to right ventricular inlet in the other patient. Finally deployment of device was successful in 57 (90.5%) and failed in 6 (9.5%). The embolized and dislocated devices were retrieved at surgery and the ASD repaired at the same time without any further complications. Follow up: In majority (61.4%) of the patients, there was a diffuse mesh leak through the central portion of the device at the end of the procedure. By the time of discharge, 24 hours after ASD closure, the rate of residual shunt had decreased to trivial residual shunt in 10 (17.5%), small residual in one (1.8%) and moderate residual shunt in two (3.5%) shunt in 10 (17.5%), small residual in one (1.8%) and moderate residual shunt in two (3.5%) patients. At 24 hour, 1 month, 6 month and 1 year follow up, total occlusion rate was 73.6%, 91%, 94.7%, and 94.7% respectively. The minor complications included transient sinus tachycardia in 10 and paroxysmal supra ventricular tachycardia in two patients, which successfully terminated with adenosine and verapamil. All but three patients remained well at one month, 6 month, 12 month and 24 month follow up. Two patients had moderate shunt and one patient had dislodgement of device in the right atrium with moderate shunt. The dislodged device was removed at surgery and the ASD closed at the same time. Discussion Transcatheter closure of ASD with Amplatzer septal occluder has replaced routine surgical repair in many centers[9]. The device is first device to receive full approval for clinical use in patients with ASD from United States Food and Drug Administration[10]. The major advantages of percutaneous closure of ASD are the absence of thoracotomy, open heart surgery and admission to an intensive care unit, thus avoiding subsequent surgical scar and post operative pain[6,11,12]. The other advantages are less psychological impact, shorter hospital stay, and less need for blood transfusion[6,11]. The absence of myocardial scar may decrease the incidence of incisional dysrhythmias[11]. Transcatheter closure of ASD is an established technique that has a low incidence of morbidity and mortality. An important advantage of the ASO is the retrievability during deployment, this greatly diminishes the risk of malposition and embolization of the device, and this reduces the risk for surgical removal of embolized devices. The deployment is performed using low profile (7-12Fr) sheath, which facilitates its use in young children. Selection of correct size of the device is important. This depends on accurate assessment of the stretched diameter of the ASD, as the device is matched to the size of the stretched ASD diameter. Oversized device can cause distortion of the retention discs and impinging on sensitive structures, while undersized device may result in residual shunting early or even late embolization of the device. Another important and essential aspect of echocardiography monitoring the procedure is to ensure positioning of device before and after its release. In our study the device was implanted with TTE monitoring without increasing the chance of embolization or dislocation. TTE is a satisfactory technique in case selection before transcatheter closure of ASD. Transcatheter closure of ASD guided by TTE is sufficient and safe, especially in children with good imaging windows[13-15]. However, sometimes TEE is impossible for technical or anatomical reasons especially in children and adolescents. The design of the device and method of fixation make it possible to close large defect with smaller rim[16]. In this series largest ASD size was 34mm and smallest rim was 4mm. This defect was closed with Amplatzer device No 36mm. In our study closure rate was 94.7% which, with regard to other reports, was acceptable[9,11,17-19]. In general the complication rate of transcatheter ASD closure is low[7,20,21]. Although the procedure itself is considered to be safe and the Amplatzer device rarely causes problems during follow up, some complications have been reported. The first problem is that the device may be embolized. Like in other reports[17,18,22], in our series, device embolization/malposition was common-est major complication, and the next common complication was arrhythmia[17,18,19,23]. Arrhyth-mias are known to be infrequent in transcatheter closure of ASD[24]. These complications are transient and benign, and are well controlled medically or recover spontaneously[18,25,26]. Mild mitral regurgitation following device implantation occurred in one patient (a child of 4.5 years age and 15 kg body weight). At 1 month follow up mitral valve became competent. Mitral valve regurgitation may occur in the patient with a small rim needing a large Amplatzer device. It usually is not progressive and has benign clinical course[27]. In our study, one patient was a 2.2 year old female, weighing 7kg. She had Down's syndrome, recurrent pulmonary infections, growth retardation and mild pulmonary hypertension. Transcatheter closure of ASD is efficient in children weighing 15 kilograms or less, and can be proposed as a first line treatment in symptomatic patient[28,29,30]. Our results demonstrate that the Amplatzer device is particularly useful in children and adolescent with the secundum ASD. Also previous studies have reported that transcatheter closure of ASD with Amplatzer is safe and effective and currently can be considered an alternative to surgical treatment for selected patients [26,31,32]. َAs a limitation of our study can be maintained that it represents single operator experience at one tertiary cardiovascular center. Conclusion Transcatheter closure of ASD in children and adolescent patients has high success rate with excellent safety documented during immediate, short to midterm follow up. Our finding suggests that Amplatzer device closure of ASD in children and adolescents should be the first option of management. However, long-term follow up is required in order to draw firm conclusion Acknowledgment This study was supported in part by a grant from the Yazd Cardiovascular Research Center. We gratefully acknowledge Dr. Majid Dehghan, who helped to establish the procedure in Afshar Hospital, Yazd. We thank Mr. MH Ahmadieh for collecting data and statistical analysis. Also the authors would like to thank the research ethics committee of Shahid Sadoughi University of Medical Sciences. Conflict of Interest: References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11029t1.jpg] [pe11029f1.jpg] [pe11029f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}