 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 2, Apri l-June, 2011, pp. 173-180 Comparison of the Effect of Fentanyl, Sufentanil, Alfentanil and Remifentanil on Cardiovascular Response to Tracheal Intubation in Children Seyed-Mohamad Mireskandari1,2, MD; Navid Abulahrar1,3, MD; Mohamad-Esmaeil Darabi1,2, MD; Iman Rahimi1,2, MD; Fatemeh Haji-Mohamadi1,4, MD; Ali Movafegh1,3, MD
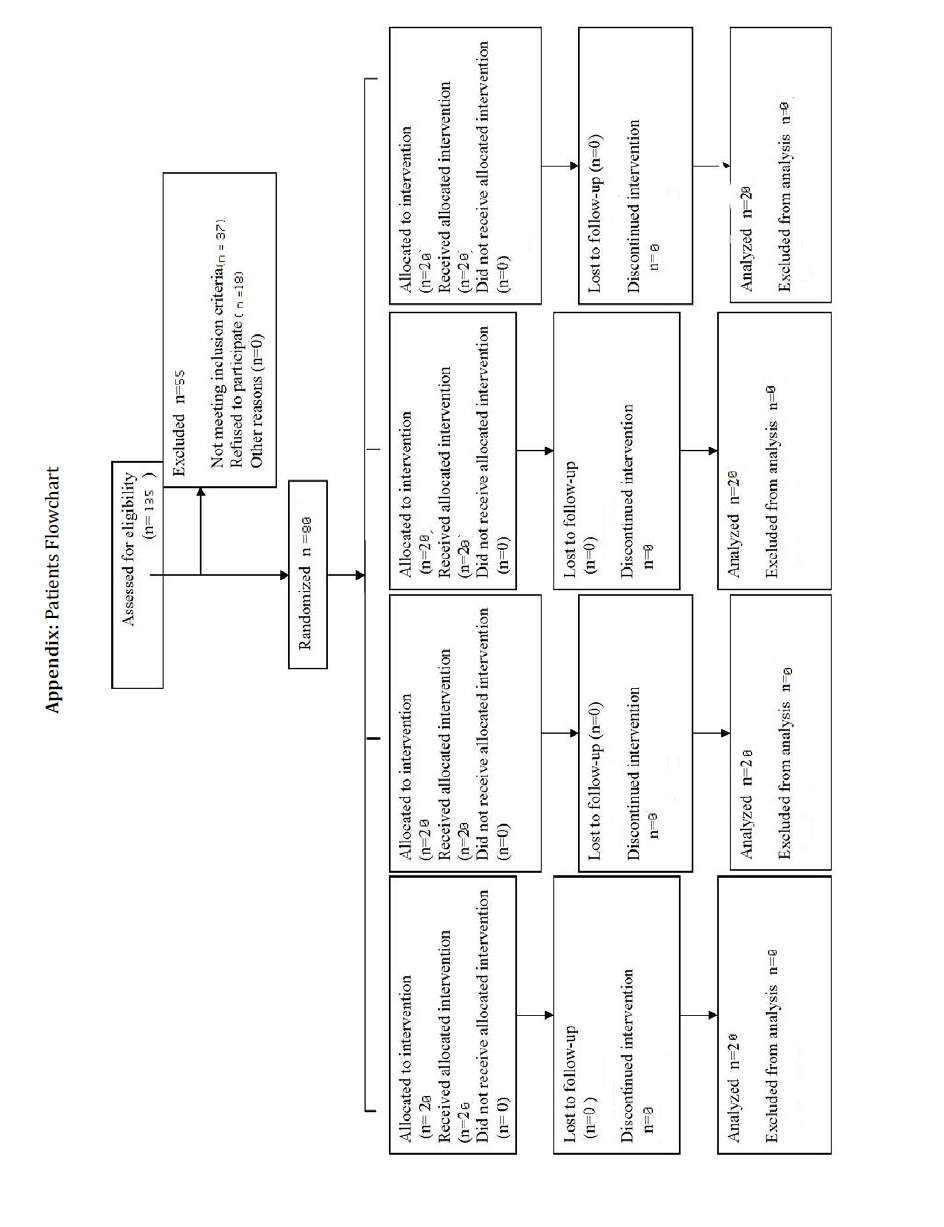
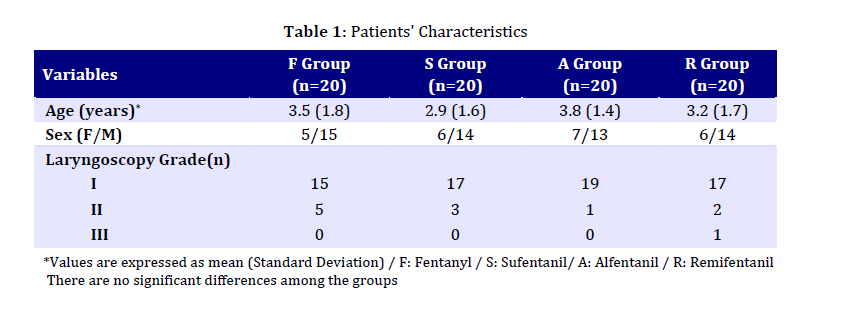
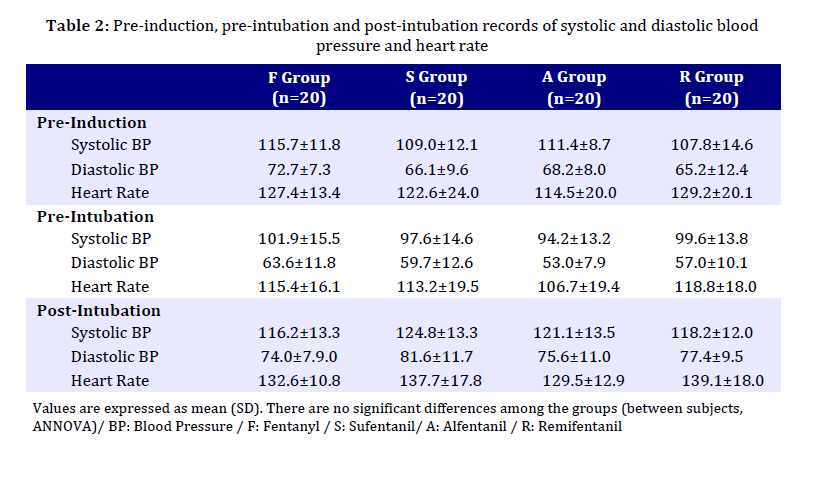
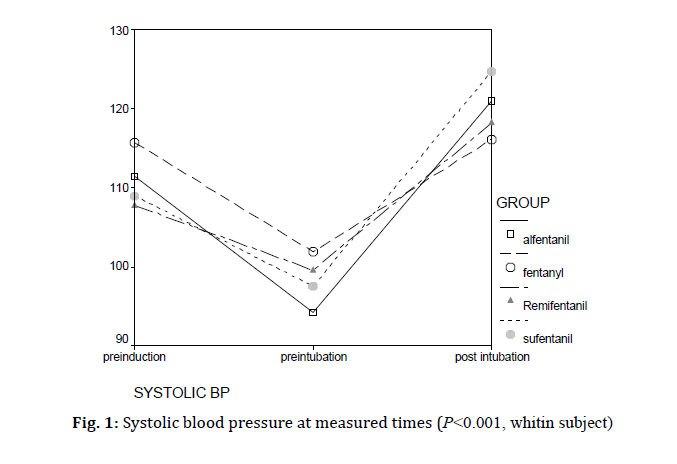
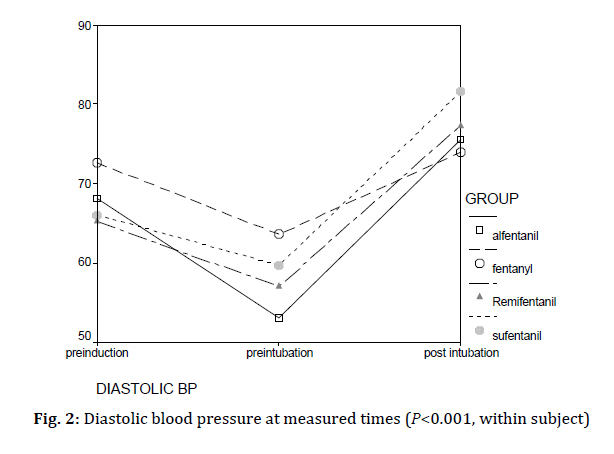
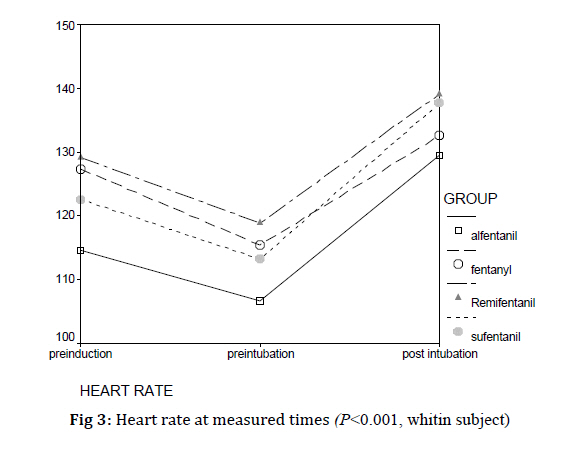
Received: Apr 10, 2010; Final Revision: Jan 10, 2011; Accepted: Feb 01, 2011 Code Number pe11030 Abstract Objective: Laryngoscopy and tracheal intubation may cause significant cerebral and systemic hemodynamic responses. Many drugs have been shown to be effective in modifying these hemodynamic responses, including fentanyl, sufentanil, alfentanil and remifentanil. The purpose of the current study was to compare the efficacy of fentanyl, sufentanil, alfentanil and remifentanil on blunting cardiovascular changes during laryngoscopy and intubation in children. Key Words: Intubation; Laryngoscopy; Opioid; Sufentanil; Alfentanil; Fentanyl; Remifentanil Introduction The peri-intubation period is one of the most stressing moments of general anesthesia. Laryngoscopy and tracheal intubation may cause significant cerebral and systemic hemodynamic responses, including tachycardia, hypertension and increased intracranial pressure[1]. Many drugs have been shown to be effective in modifying these hemodynamic responses in children including fentanyl, sufentanil, alfentanil and remifentani[2-9]. These potent synthetic opioid drugs are frequently used in adult anesthesia; however, to the best of our knowledge, no single study has compared these four opioids together and their effects on cardiovascular changes during laryngoscopy and intubation in children. The purpose of the current study was to compare the efficacy of fentanyl, sufentanil, alfentanil and remifentanil on blunting cardiovascular changes during laryngoscopy and intubation in children. Subjects and Methods The protocol was approved by the Institutional Ethics Committee and informed written consent was obtained from the patient’s parents. Eighty children, 1-6 years old, classified as American Society of Anesthesiologists physical status I and II who were scheduled for elective surgery with general anesthesia and oro-tracheal intubation and no difficulties with their airway or intubation were predicted during preoperative visits, were enrolled in this randomized and double-blinded study. Patients with a history of cardiovascular disorders and those who received any medication in 48 hours before surgery were not enrolled in the study. Patients were randomly assigned into four groups of either fentanyl (Group F, n=20), sufentanil (Group S, n=20), alfentanil (Group A, n=20) and remifentanil (Group R, n=20) using a computer generated randomization list. Before surgery, all children fasted overnight and were restricted from oral intake of clear fluid for 2–3 h. Ninety min before transferring children to the operating room, an intravenous access on the dorsum of a hand was established using a 22-gauge catheter inserted in the surgical ward 45 min after the application of EMLA cream and then the patients received midazolam 0.1 mg/kg-1 orally. In the operating room, an infusion of lactated ringer’s solution was commenced. All patients were monitored with an electrocardiogram (ECG), non-invasive blood pressure and pulse oximetry. Patients in group F received fentanyl 1µg/kg-1, in group S received sufentanil 0.1 µg/kg-1, in group A received alfentanil 10 µg/kg-1 and in group R received remifentanil 1 µg/kg-1 intravenously. Then, anesthesia was induced with propofol 2.5 mg/kg-1 and muscle relaxation by cisatracurium 0.2 mg/kg-1 administered IV over a 30s period. When a response to verbal command was absent, child was ventilated via facemask with 100% oxygen. If any difficulty was encountered in performing facemask ventilation, the child was excluded from the study. After establishment of neuromuscular blockade, confirmed with a nerve stimulator, laryngoscopy and orotracheal intubation were performed 3 min after induction. During intubation, the child’s head was placed in the sniffing position. The intubations were performed by using a Macintosh laryngoscope by experienced anesthesiologist while the patient was in the sniffing position. Children who required more than one attempt to achieve successful intubation were excluded from the statistical analysis of data. Ventilation was adjusted to maintain normocapnia (end-tidal carbon dioxide partial pressure 4.7-5.3 kPa). Patients were actively warmed to keep core temperature (esophageal) normothermic. A polyvinyl-chloride uncuffed tracheal tube was used in this study. The suitable size of tracheal tube was determined by the formula (age+16)/ 4. Hemodynamic variables including systolic and diastolic blood pressure (SAP, DAP), heart rate (HR) were recorded at base line (before opioids administration), before laryngoscopy and one minute after orotracheal intubation. All drugs were prepared by an anesthetist who was not involved in the anesthesia administration nor in patient observation in the similar syringes, thus, both the anesthesiologist and the patients were blinded to the group assignment. Escape medication (ephedrine 0.05 mg/kg-1 in increments) was administrated for hypotension (SAP<70 mmHg or a decrease of >30% of baseline values for >60s) and atropine 20 µg/kg-1 in increments for bradycardia (HR<60 min-1). It was estimated that a minimum of 18 patients in each group would be required to have a 95% power of detecting a 15% difference at a significance level of 0.05, and this number has been increased to 20 per group, to allow for a predicted drop-out from treatment of around 10%. Statistical analysis was performed using SPSS package version 13.5 (SPSS Inc., Chicago, IL, USA). The distribution of age, weight, laryngoscopy Cormack and Lehane grade, systolic and diastolic blood pressure and heart rate was checked by the Kolmogorov-Smirnov test. They followed a normal distribution. Age and weight were compared between four groups by one way ANOVA. To compare the SAP, DAP and HR changes between four groups in each time of measurement, repeated measure analysis of variance were used. Two tailed P<0.05 was taken as significant. Findings We randomized 80 patients. There were no protocol violation and all patients were included in the analysis. The consort flowchart was showed in appendix. Patients' characteristics and laryngoscopy grade were similar in all groups (Table 1). There was no significant difference in the mean values of SAP, DAP and HR at each measured time between the four groups (Table 2). There was significant difference in the mean values of SAP, DAP and HR measured over time in each group (repeated measure analysis of variance, within subject effect, P<0.001) (Fig. 1, 2, and 3). The mean value of SAP and DAP in fentanyl and sufentanil groups showed the least and greatest changes, the mean value of the SAP (and DAP) in fentanyl group was 115.7 (and 72.7) mmHg at pre-induction period, droped to 101.9 (and 63.6) mmHg at pre-intubation period and again raised to 116.2 (and 74) mmHg at post-intubation period. In sufentanil group, the mean value of the SAP (and DAP) changed from 109.0 (and 66.1) mmHg at pre-induction to 97.6 (and 59.7) mmHg at pre-intubation and finally to 124.8 (and 81.6) mmHg at post-intubation periods (Fig. 1 and 2; P<0.001). HR changes were minimum in fentanyl but maximum in alfentanil group. In fentanyl group, HR at pre-induction, pre-intubation and post-intubation periods were 127.4, 113.4 and 132.6 min-1, respectively. In Alfentanil group, HR dropped from 114.5 min-1 at pre-induction period to 106.7 min-1 at pre-intubation period, and rose to 129.5 min-1 at post intubation period (Fig. 3, P<0.001). Discussion The current study demonstrates that in children intravenous fentanyl 1 µg/kg-1, sufentanil 0.1 µg/kg-1, alfentanil 10 µg/kg-1 and remifentanil 1 µg/kg-1 comparably attenuated pressor responses to laryngoscopy and intubation. However, hemodynamic stability was significantly better preserved with fentanyl. Induction of anesthesia and tracheal intubation may induce profound alternation of the hemodynamic state according to both the effects of anesthetic drugs administrated perioperatively, and the adrenergic state of the patient[10]. Many pharmacological strategies have been proposed to blunt cardiovascular responses during intubation, including the use of topical, nebulized local anesthetics, the use of beta blockers, or other cardiovascular drugs. Opioid administration is the most extensively used strategy[10]. Fentanyl is the most commonly used narcotic in infants and children[11]. Fentanyl has also provided more stable pressor responses to intubation than remifentanil in nom-paralyzed children[2]. Sufentanil can result in a dose-related attenuation of the cardiovascular intubation response, with 0.3 µg/kg-1 as the optimal dose[9] with less cardiovascular depression. Sufentanil 0.2 µg/kg-1 has still been superior to fentanyl 2 µg/kg-1 in paralyzed children without premedication with midazolam[8]. However, we found sufentanil 0.1 µg/kg-1 subjacent to fentanyl 1 µg/kg-1. This can be explained by: 1) better performance of fentanyl at such low doses, 2) advantage of premedication with midazolam that serves low dose fentanyl better than low dose sufentanil 3) merely chance Remifentanil has been suggested to provide adequate intubating conditions at 3-4 µg/kg-1 in absence of neuromuscular blockade[12-15] and at 0.5-2.0 µg/kg-1 in presence of neuromuscular blockade[3,5,16-20]. However, remifentanil has been associated with bradycardia and hypotension even at doses as low as 0.5 µg/kg-1; therefore pretreatment with either atropine or glycopyrrolate has also been suggested[4,10,17,20]. Alfentanil, which is not well studied in children, has also been suggested to provide suitable intubating conditions and hemodynamic responses to intubation in adults at 36-40 µg/kg-1[14,21]; however it is accompanied with noticeable bradycardia even at doses as low as 15 µg/kg-1 [22]. We didn’t use any vagolytic premedication to avoid a bias; however we did not face with bradycardia in any group at all. Remifentanil and sufentanil have comparable and satisfactory effects on hemodynamic responses to intubation either at 0.1 µg/kg-1 and 0.01 µg/kg-1 respectively[10] or 1 µg/kg-1 and 0.1 µg/kg-1 respectively[16] in neuromuscularly blocked adults when premedicated with midazolam 0.05 mg/kg-1. We did also find comparable effects of remifentanil 1 µg/kg-1 and sufentanil 0.1 µg/kg-1 in our premedicated and paralyzed children. Xue and colleagues have avoided premedication in their two recent studies[8,9] to exclude a bias. They have referenced an old study where adults patients premedicated with hyoscine before rapid sequence induction of anesthesia with sufentanil and suxamethonium had a significantly higher mean heart rate and mean arterial pressure than patients premedicated with lorazepam[23]. However in balanced anesthesia, premedication with almost all sedatives has the advantage of reducing anesthetic requirements and blunting pressor responses to intubation; notwithstanding it is especially warranted in a fearful child. Oral midazolam is the most commonly administered premedication in the United States[24] and generally results in very compliant children who will separate from their parents without crying[25]. We applied our routine clinical doses for the studied opioids in our paralyzed and premedicated children, who received propofol for induction on anesthesia. Other individual dose finding studies[3-6,9,13,18-22,26,27] or comparative studies[2,8,12,14-17], while mostly in adults and scarce in children, were not congruent in use of midazolam as premedication, atropine or glycopyrrolate, neuromuscular blockade, and in induction of anesthesia; and none had compared all the four opioids together. Present study had a few limitations. In this study, the serum level of the study drugs was not measured. Moreover, only one dose of each drug was administrated, so further dose finding studies with more study groups recruited and larger sample sizes of neuromuscularly blocked pediatric patients premedicated with midazolam may reveal optimal doses of an ideal opioid and the need for pretreatment with a vagolytic during laryngoscopy and intubation. Conclusion Our findings demonstrate that in children intravenous fentanyl, sufentanil, alfentanil and remifentanil comparably attenuated pressor responses to laryngoscopy and intubation and hemodynamic stability was significantly better preserved with fentanyl. Acknowledgment The proposal of this manuscript approved in the research committee of the department of anesthesiology and critical care of Tehran University of Medical Sciences, and registered in the Iranian Registry of Clinical Trials with following number: IRCT201012025175N4 Conflict of Interest: There was no conflict of interest in this study References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11030f2.jpg] [pe11030f1.jpg] [pe11030f3.jpg] [pe11030t2.jpg] [pe11030t1.jpg] [pe11030a1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}