 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 2, Apri l-June, 2011, pp. 188-192 Does Congenital Hypothyroidism Have Different Etiologies in Iran? Zohre Karamizadeh1, MD; Setillia Dalili1, MD; Heidyeh Sanei-far1, MD; Hamdollah Karamifard1, MD; Hamid Mohammadi2, MD, and Gholamhossein Amirhakimi1, MD
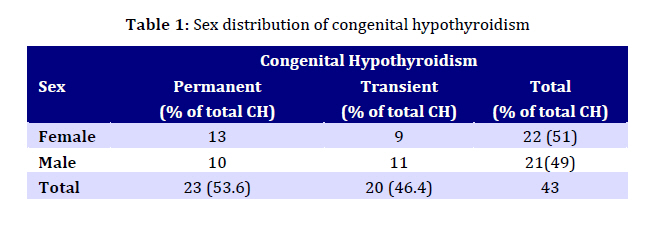
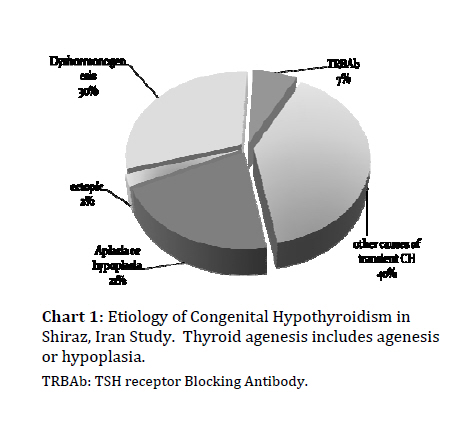
Received: Feb 15, 2010; Final Revision: Oct 05, 2010; Accepted: Dec 26, 2010 Code Number: pe11032 Abstract Objective: To determine the prevalence of congenital hypothyroidism (CH), permanent and transient CH. Key Words: Congenital Hypothyroidism; TSH Receptor; Dyshormonogenesis; Thyroid Dysgenesis Introduction Congenital hypothyroidism (CH), one of the most common pediatric endocrinological diseases results from the dysfunction of the thyroid gland and if untreated may lead to serious impaired mental and physical development[1]. Thyroid hormone is important for normal development of the nervous system[2,3]. Severe hypothyroidism is seldom apparent at birth and a systematic screening for congenital hypothyro-idism is required. Congenital hypothyroidism has a prevalence of 1/4000 to 1/3000 in newborns [4]. This number varies depending on the race/ethnicity and the method of screening [5]. The need for thyroid hormone supplementation can be permanent or transient. In approximately 85% of affected newborns, permanent primary congenital hypothyroidism is due to thyroid dysgenesis and 15% due to defects in thyroid hormone biosynthesis (thyroid dyshormonogenesis), which because of the trophic action of thyrotropin, eventually leads to thyroid enlargement. This thyroid enlargement is very often not detected clinically at birth. The rare causes of permanent hypothyroidism include resistance to thyrotropin, central hypothyroidism, developmental defects, inactivating mutation, abnormal thyroid hormone transport into the cell and thyroid hormone resistance[6,7]. Transient CH can be caused by iodine deficiency, perinatal exposure to excess iodine (e.g. use of iodinated disinfectants or contrast agents) or fetal exposure to either maternally derived thyroid blocking antibodies or anti-thyroid drugs taken by pregnant women with autoimmune thyroid disease[8]. The aim of this study was to determine the incidence of permanent and transient CH among neonates with diagnosis of CH in Shiraz screening program. Subjects and Methods Between November 2006 and September 2007 all neonates who were screened in Fars province, South Iran and had a thyroid stimulating hormone (TSH) level equal to or greater than 5mU/L were referred to the pediatric endocrinology clinic. The screening test was performed by TSH measurement on a filter paper blood spots and sampling was carried out between 3 to 5 days after birth. For all patients, family history, gestational age, birth weight, and history of jaundice or blood transfusion were recorded and a complete physical examination was done (weight, height, head circumference, size of anterior and posterior fontanels and presence of umbilical hernia). Serum TSH, T4 and TSH receptor blocking antibody (TRBAb) were measured and recorded. Neonates with confirmed hypothyroidism underwent treatment with a single dose of levothyroxine (10-15 mgr/kg/day). Neonates with CH underwent thyroid scintigraphy with technetium pertechnetate to determine the etiology of hypothyroidism. Thyroid ultrasonography was performed when scintigraphy did not show any uptake in the thyroid gland area to confirm thyroid agenesis. Infants diagnosed with CH were followed closely for the first three years of life. They were followed every one to two months during the first year of life and every two to three months during the second and third years. In order to distinguish between permanent and transient CH, around 3rd year of follow up, levothyroxine therapy was discontinued for 4 weeks in CH cases except in those with elevated serum TSH during 6-12 months of levothyroxine therapy and/or confirmed thyroid dysgenesis. Then patients were reevaluated by serum TSH and T4 measurement. Thyroid sonography was also performed in all patients around this time. All patients with TSH levels >6 mU/L after 4 weeks of levothyroxine discontinuation were diagnosed as a permanent congenital hypothyroidism. TSH receptor blocking antibody was also measured in all mothers during follow up period. TSH was measured by immunoradiometric assay (IRMA) (Xit Immunotech, Belgium). T4 was measured by radioimmunoassay (RIA) (Immunotech, Blegium) and TRBAb by Elisa (Diametera, Italy) and TRBAb values greater than 1.5 m/l were considered abnormal. Findings Between November 2006 and September 2007, a total of 63,031 neonates were screened in Fars province and 127 neonates (about 1:500 of screened neonates) with an abnormal screening result were referred to the pediatric endocrinology clinic. In 43 cases, CH was diagnosed with a prevalence of 1:1465. Sex distribution of these 43 patients was 51% (22 cases) females and 49% (21cases) males (table 1). Regarding the total number of screened females and males, the incidence of CH was 74 and 64 in 100000 births respectively. The clinical findings included: 31 (73.1%) neonates with CH had a history of prolonged jaundice, 5 (11.6%) an umbilical hernia, 23 (55%) large posterior fontanel (>0.5 cm) and 24 (56%) large anterior fontanel (larger than 2.5×2.5). None of the patients had a history of CH or thyroid disease in his/her mother or siblings. Parental consanguinity was present among 34.1% of confirmed congenital hypothyroidism patients. The incidence of permanent and transient hypothyroidism was 53.6% (23 cases) and 46.4% (20 cases) respectively according to the scintigraphic and/or ultrasonographic findings. Among 20 patients with transient CH, 7 patients had elevated TSH level and normal T4 (“isolated hyperthyrotropinemia”). TRBAb: TSH receptor Blocking Antibody. All patients with transient CH had normal thyroid glands and in permanent CH 13 cases (57%) had dyshormonogenesis, 10 cases (43%) had thyroid dysgenesis (9 cases of agenesis or hypoplasia and 1 case of ectopia). The mean TSH values in transient CH were significantly lower than those in patient with permanent CH (27.2 versus 60.3 with P value <.001). Three out of 43 CH infants were found to have TRBAb; this suggests that the prevalence of CH due to TRBAb was 6.9%. The maximum serum TRBAb in CH group was 23.5u/L and minimum level was 5u/L. Discussion In the present study screening of CH was done in Fars province between November 2006 and September 2007 to evaluate the incidence and etiology of congenital hypothyroidism. Among a large number of screened neonates 127 cases had abnormal screen tests, and among this population, 43 (35%) neonates had a definite diagnosis of CH that indicates an incidence of 1:1465 in Fars, Iran. This is comparable to other studies that report an incidence of 1:1300 [9] (in the Netherlands) or 1:1800 in Thailand[10] and Lebanon[11]. Interestingly, other studies in Iran show a higher incidence 1:357 in Isfahan[12] by Hashemipour et al, and 1:914 in Tehran, Ordookhani et al. Both studies used the same method and material for case finding based on national screening programs in Iran. Hashemipour et al relate the higher incidence to “dissimilarity between the screening methods, environmental, genetic and immunologic factors”. As screening methods and genetic factors in the present study are the same as in other studies in Iran, so environmental factors may play a more prominent role in the incidence and prevalence of CH. Although the female/male ratio in this study was 1.19:1, there was no statistically significant difference. On the other hand in most articles, female to male ratio is around 2/1[13,21]. In this study, the difference may be related to different etiologies of CH that reveals dyshormonogenesis as the most prevalent cause of CH and a higher rate of transient CH. In this study of 43 patients with CH, 53.6% and 46.4% were confirmed to have the permanent and transient form of the disorder respectively. This finding is similar to that of other authors in Iran such as Hashemipour et al that report 59.8% permanent and 40.2% transient CH[12]. Some other studies report a reverse ratio; Caudino et al found 38% and 62% of 79 patients with CH as transient and permanent CH, respectively[14], others report the incidence of transient CH as 5% to 10% of infants in newborn thyroid screening programs[15,17]. Considering the etiologies of transient CH, further investigation is needed to rule out iodine deficiency in our population. Most of these transient cases had a disease duration longer than 4-5 months, so maternal drug use or maternal blocking antibodies are less likely to be the cause of higher rate of transient CH in this study. In addition to these probable causes, it seems that longer follow up for a case with transient hypothyroidism is required. Because some of our patients with normal TSH after one month of drug withdrawal (transient CH) had a rise of TSH 4-5 months later that lead to diagnosis of permanent CH. Another noticeable point are patients with high TSH and normal T4; Muge Tamam et al reported 17% of 182 patients as “Isolated Hyperthyrotropinemia”, that were neither transient nor permanent cases of CH[16]. They recommend that these patients can be followed without hormone therapy. Some of our patients (35% of transient cases and 17% of total CH cases) had same laboratory features also. In this study and most probably in other studies in Iran these cases were labeled as transient hypothyroidism. We believe that this is a major factor for a higher rate of transient CH in our study. In most articles and book reviews dysgenesis of thyroid gland is the most common cause of CH and dyshormonogenesis being the next one[17], but our results differ and show 57% dyshormonogenesis and 43% dysgenesis as etiologies of permanent CH. Interestingly thyroid agenesis was also more prevalent than thyroid ectopia among patients with thyroid dysgenesis. Another study in Isfahan, Iran by Hashemipour et al also reported 58.8% and 42.2% as prevalence of dyshormonogenesis and dysgenesis respectively and higher rate of agenesis than ectopia[12]. Some similar results in other countries are also reported, such as the study of Eugster D et al that reveals that dyshormonogenesis was more prevalent (57.1% of permanent CH)[15]. These findings need more studies to find other possible etiologic factors for CH in Iran. In this study the mean TSH level before treatment was significantly higher in patients with permanent CH than in those with transient CH (P<0.001 and a ratio 3.0) as reported by multiple studies in this field[15,17,18]. We screened neonatal blood to estimate the incidence of TRBAb induced CH. The incidence of TRBAb based on neonatal serum analysis for thyroid receptor blocking antibody was 6.9% (3 cases); that is slightly more than that of other studies and may be due to small size number of cases with CH, but there are no other studies available in Iran for comparison. Brown RS et al, report 2% and Mengreli C et al 2.7% as incidence of TRBAb[18,19] in their studies. Lafranchi S reported an incidence of 5% for CH due to maternal TRBAb[20]. Conclusion Congenital hypothyroidism in Iran may have different etiologies, so more and larger studies are needed to find clear information about the incidence, prevalence and etiologic factors of this disease. Transient CH has a significantly higher rate than other similar studies. It is reasonable to recommend following these patients for a longer period to rule out probable permanent hypothyroidism that may be detected a few months after drug withdrawal. Acknowledgment We acknowledge the contribution of Dr A. Banihashemi in preparing this manuscript and Clinical research development center of Nemazee hospital for statistical analysis. We used some data of national screening program of hypothyroidism as total number of screened cases and referral cases. Conflict of Interest: No conflict of interest was noted in this research. References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11032t1.jpg] [pe11032f1.jpg] |
| |||||||||

{kind=link}
{kind=link}