 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 2, Apri l-June, 2011, pp. 220-224 The Relationship between Coronary Artery Aneurysm and QT Interval Dispersion in Acute Phase of Kawasaki Disease Abdolrazagh Kiani1, MD; Sima Rafieyian, MD; Shahla Roodpeyma2, MD; Maryam Sefidgarnia, MD
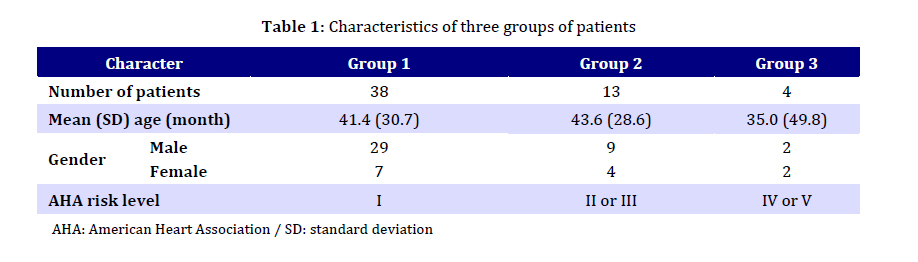
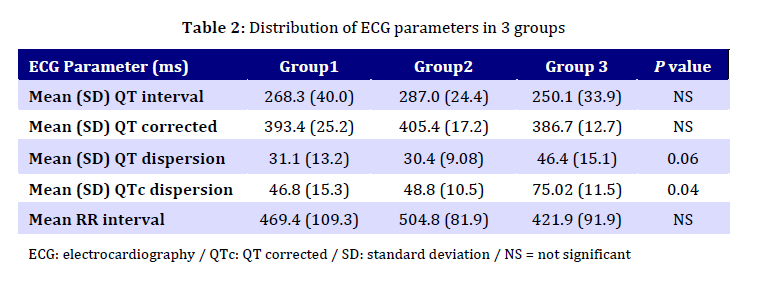
Received: Jul; 21, 2010; Final Revision: Jan 10, 2011; Accepted: Jan 15, 2011 Code Number: pe11037 Abstract Objective: QT dispersion (QTd) has been proposed as a marker of ventricular repolarization inhomogeneity and several investigations have proved the relationship between it and cardiac ischemia, ventricular arrhythmia and sudden cardiac death. The aim of this study was to assess the relation between coronary artery involvement and QTd, and QTc dispersion (QTcd) in the acute phase of Kawasaki disease (KD). Key Words: Coronary Artery Aneurysm; Kawasaki Disease; QT Dispersion; Cardiac Arrhythmia; ECG Introduction Kawasaki disease (KD) is the most prevalent inflammatory coronary artery disease. It is a leading cause of acquired heart disease in children[1]. Coronary artery involvement remains the most important complication of KD and involves a continuous spectrum ranging from no apparent involvement in the majority of patients to the presence of multiple giant aneurysms[2-4]. Coronary artery dilatation or aneurysms develop in approximately 25% of untreated children with KD and may lead to myocardial infarction, sudden death, or ischemic heart disease[5]. Early diagnosis and treatment with intravenous immunoglobulin (IVIG) can reduce the incidence of coronary artery abnormalities to <5%, while primarily an acute, multisystem vasculitis is more appropriately described as a pancarditis, from cardiac perspective[6,7]. Ventricular dysfunction and arrhythmias also occur, and may be independent of coronary artery involvement[8]. This may be indicated by echocardiographic (echo) abnormalities in ventricular dimension and functions, and electrocardiographic (ECG) abnormalities in ventricular forces and repolarization. The relationship between possible markers of myocardial inflammation and the degree of coronary artery abnormalities has not been well characterized[9]. Increased QTd has been associated with an increased risk for ventricular arrhythmia and sudden cardiac death. The dispersion is indicative of inhomogeneous ventricular repolarization and may represent increased risk for developing ventricular arrhythmia in this population [10]. Our purpose in the present study was to evaluate the coronary artery involvement in a group of Kawasaki patients. We wanted to find the relationship between the coronary artery involvement and the QTd in this group of patients. Subjects and Methods The study was conducted at Children's Medical Center, a tertiary referral center of Tehran University. The records of all children with a discharge diagnosis of KD were collected retrospectively between 2006 and 2009. The diagnosis of KD was based on American Heart Association Criteria[7]. The medical records of all patients were reviewed to obtain data regarding demographic, clinical features, ECG, and echo measurements. The majority of children presented within 10 days after onset of fever. The degree of coronary artery involvement was classified according to the Japanese Ministry of Health Criteria[11]. The coronary artery internal diameter of 3 to 8 mm in children <5 years of age or 4 to 8 mm in children ≥5 years old was defined as small to medium size aneurysm. The internal diameter of ≥8 mm was defined as giant aneurysm. Multiple small to medium size aneurysms, obstruction or thrombosis of coronary arteries were also considered as severe involvement. Echocardiographic assessment of coronary arteries was in parasternal short axis view. According to condition of coronary artery and American Heart Association (AHA) risk level[12] patients were divided into three groups. Patients without coronary artery involvement were classified as group I with AHA risk level 1. Patients with small to medium size aneurysm were classified as group II with AHA risk level II or III. Patients with giant aneurysm, and/or severe involvement were placed in group III with AHA risk level of IV or V. For each patient, a 12 leads ECG with one channel was recorded at a speed of 25 mm/sec by ECG machine Fokuda (Japan) during the acute phase of disease. QT interval was measured from the beginning of QRS complex to the end of T wave for 2 cycles of each lead. The end of T wave was defined as the point of return to base line, and in the rare occasions of presence of a U wave, the U wave was not included and the T wave was extrapolated to base line. The RR interval was measured for each cycle and QT corrected interval (QTc) was calculated by using the Bazzet's formula (QTc = QT/square root of the RR interval). QTd was calculated as the difference between the minimum and maximum QT intervals for any of the 12 leads, and QTc dispersion was calculated accordingly. Measurements of recording were made by using hand caliper and by a single trained observer. Data of the three groups were compared by Chi-Square test and P<0.05 was considered significant. The ability of QTd ≥50 ms and QTd ≥60 ms to detect severe coronary artery involvement was defined as sensitivity and positive predictive value was measured by true positive results/total positive results ×100. The ability of QTd ≥50 ms and QTd ≥60 ms to define absence of severe coronary artery involvement was defined as specificity and negative predictive value was measured by true negative results/total negative results ×100. The study was approved by ethical committee of the hospital. Findings During the 3-year study period, we had 65 patients with discharge diagnosis of KD. Of the 65 cases, 40 (61.6%) were males and 25 (38.4%) females. Our patients’ ages ranged from 3 to 138 months with a mean of 41.46+31.11 months. Forty eight patients without coronary artery involvement were classified as group 1. Group 2 and 3 consisted of 13 and 4 patients respectively. Table 1 shows the characteristic of each group. Table 2 summarizes the ECG parameter measurements in 3 groups. As it is shown in this table the QTd was higher in group 3 than in group 1 and 2 (46.46±15.17 ms vs 30.44+9.08 ms, and 31.11±13.27 ms respectively), but the difference was not statistically significant (P=0.06). QTcd in group 3 was significantly greater than that in two other groups (75.02±11.53 ms vs 46.82±15.39 ms and 48.88±10.55 ms respectively, P=0.04). There was no significant difference between 3 groups in respect to QT and QTc measurements. For detecting severe coronary artery involvement, a QTd ≥50 ms had a sensitivity of 50%, specificity of 93.4%, a positive predictive value of 33.3%, a negative predictive value of 96.6%, and a diagnostic accuracy of 90.8%. When a QTcd threshold of ≥60 ms was used to detect patients with severe coronary artery aneurysm, the sensitivity was 100% (4 of 4 patients). The specificity was 93.4% (57 of 65 patients), the positive predictive value was 50% (4 of 8 patients), the negative predictive value was 100%, and the diagnostic accuracy was 93.8%. There was no evidence of arrhythmias in ECG records of our patients. Discussion On the basis of the present results we have shown that QTcd is increased in KD patients with coronary artery involvement. An ECG is useful for seeking the evidence of myocarditis[13]. Ventricular arrhythmias have been reported in the acute phase of KD independent of coronary artery involvement [14]. While systolic ventricular dysfunction may not be evident, sub clinical myocardial involvement may be indicated by subtle ventricular dilatation and repolarization abnormalities [9]. We did not find ventricular arrhythmias in our study group. It is uncertain that increased QTd would exactly indicate progression of myocardial ischemia after KD[15]. Ghelani et al examined QT interval dispersion in 20 north Indian children. The patients were in convalescent phase of KD and had not coronary artery abnormalities. The control group consisted of 20 age and sex matched healthy children. The QTd was significantly (P≤0.001) increased in children with KD[10]. The above findings indicated that increased QTd in KD is not a specific feature for coronary artery inflammation. Osada et al reported that QTd of ≥60 ms had higher sensitivity for detection of severe involvement of coronary artery after KD[15]. Our data showed that QTcd of ≥60 ms has a high sensitivity (100%) and specificity (93.4%) for detection of giant coronary artery aneurysm. Dahdah et al demonstrated that both depolarization and repolarization parameters are altered in patients with persistent coronary artery aneurysms long–term after KD[16]. The findings of the present study must be viewed in the light of some potential limitations. The present study population did not include patients with incomplete presentation, those presenting beyond 10 days from fever onset, and those not treated with IVIG. Thus, our study findings may not be completely generalized to the total population of patients being identified with potential KD in clinical practice. Conclusion Our data showed that QTc interval dispersion is significantly increased in KD children with severe coronary artery involvement. Further studies over longer follow–up period are necessary to define the implication of these findings. Acknowledgment The study was approved by local ethical committee of Shahid Modarres Hospital. Conflict of Interest: Non declared References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11037t1.jpg] [pe11037t2.jpg] |
| |||||||||

{kind=link}
{kind=link}