 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 2, Apri l-June, 2011, pp. 129-138 Atypical Presentation of Renal Angiomyolipomas in a Child with Tuberous Sclerosis Complex Pietro Ferrara1, MD; Valerio Romano1, MD; Antonio Gatto1, MD; Ottavio Vitelli2, MD; Pio Liberatore1, MD; Sofia Passera1, MD; Giorgia Bottaro2, MD; Francesca del Bufalo2, MD; Diego Martinelli1, Maria Del Re1, MD, and Domenica Battaglia1, MD
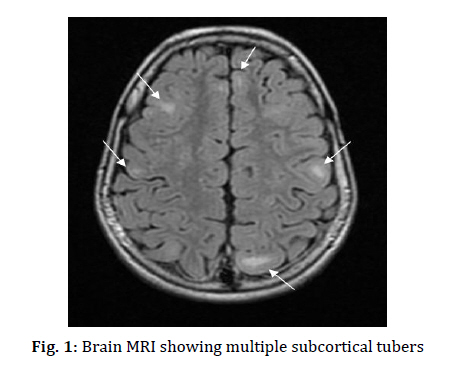
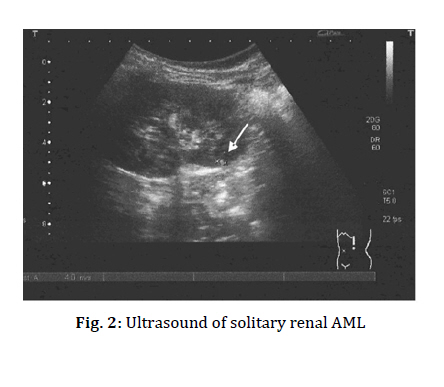
Received: Jul 14, 2010; Accepted: Jan 15, 2011 Code Number: pe11045 Key words: Micturitional Disorders; Renal Angiomyolipomas; Tuberous Sclerosis Complex Tuberous sclerosis complex (TSC) is an autosomal dominant genetic disorder with a birth incidence of 1:6.000. It can virtually affect any organ system and all racial and ethnic groups[1]. Clinical manifestations of TSC have variable penetrance. Many affected patients come to medical attention because of seizures or dermatological manifestations. Since no single feature of TSC is pathognomonic, an evaluation of all clinical features is necessary. Sparagana et al recommend, the execution of cranial imaging, such as brain magnetic resonance imaging (MRI) or computerized tomography (CT), and of renal ultrasound (US), on a 1-3 years basis. Brain tumors and renal lesions, in fact, account for most of the long-term morbidity and mortality caused by TSC[2]. Renal involvement occurs with high frequency and with a wide range of severity in patients with TSC[1,3]. Renal angiomyolipomas (AMLs) and cysts represent the most frequent findings in patients affected by TSC. We report the case of an 8-year old boy, born after a near term uncomplicated pregnancy, affected by TSC. When he was 10 months old, he presented the first episode of seizures, characterized by spasms in flexion and adduction of the upper limbs and trunk, eyes deviation, loss of consciousness and subsequent diffuse hypotonia, for about 1-2 minutes. Since two similar episodes occurred in the next few days, a video electroencephalography (EEG) was performed. Awake EEG showed asymmetrical posterior activity, with higher frequency on the right regions; slow waves on the centro-parieto-temporal areas predominant on the right regions; isolated spikes on the left centro-temporal and parietal regions. Stage II sleep EEG showed paroxysmal activities; brief multifocal and synchronous and diffuse spikes; spike-waves bursts were observed. Two months later a brain MRI showed multiple subcortical tubers consistent with the diagnosis of TSC (Fig 1). Brain MRI, EEG and abdomen US were performed every year. When he was 4 years old gastro-esophageal reflux disease (GERD) and celiac disease (CD) were also diagnosed. Micturitional disorders (MD), characterized by diurnal and nocturnal incontinence, urgency and pollakisuria, appeared when he was 6 and hospitalization was required. On physical examination the patient was apyretic, with normal hemodynamic parameters. He presented multiple hypopigmented macules and facial angiofibromas. No abdominal pain, nausea, vomiting, palpable mass, hematuria, anemia, hypertension or other significant clinical problems were present. Laboratory findings were normal. Urine analysis and urine culture were negative. The urodynamic study revealed an overactive bladder. He underwent a renal US that revealed bilateral hyperechogenic masses, one of 6 mm in the right kidney and two of 3 mm in the left kidney, consistent with the diagnosis of AMLs (Fig 2), which was not shown in the previous renal US 6 months earlier. Renal lesions were managed by watchful waiting, performing a renal US after 6, 12 and 24 months and then every year. During the follow-up period the masses have been essentially unchanged in size. However, MD did not respond to therapy with desmopressin and oxybutynin. Most patients affected by TSC, exhibit primarily dermatological, renal, and neurological problems. Other clinical manifestations include lymphangioleiomyomatosis, cardiac rhabdo-myomas and retinal astrocytic hamartomas[4]. We did not find evidence of association between TSC, presenting with renal AMLs, and CD or GERD in the literature. Symptoms of AMLs are often absent or minimal, but symptomatic patients may present painless hematuria, flank pain, or retroperitoneal bleeding which leads to shock in one-third of the cases[5]. Our patient initially came to our attention for the onset of seizure, he has been followed up every year with brain MRI, video-EEG and abdominal US. A renal US was performed as a consequence of the onset of micturitional disorders, revealing bilateral renal AMLs. AMLs was differentiated from other fat-containing kidney tumors only by US since, as described by Shin et al, the presence of a hyperechogenic fat lesion in the context of the kidney without calcifications is suggestive of AMLs and need no further radiological evaluations[6]. Moreover, Siegel et al in their retrospective study comparing the ultrasound characteristics of AML and renal cell carcinoma (RCC) suggest that a hyporeflective rim and/or intra-tumoural cysts are highly suggestive of RCC[7]. In the same study, acoustic shadowing was seen in 33% of AMLs and in no RCCs. A separate study evaluating small renal lesions (<3 cm) found that a lower number (21%) of small AMLs cast an acoustic shadow, but confirmed that no RCCs examination had this appearance. The hyperechogenic nature of AMLs is likely due to a combination of fat content, blood vessels and its heterogeneous nature. RCC instead presents a hyporeflective mass and could be associated with cysts[7]. In our patient, the fear of malignancy would have remained if a minimal-fat AML or cysts were present. Finally we underline that the onset of renal AMLs could be associated to abnormal urological manifestations. Through this case report we suggest that it is necessary a more exhaustive study of kidneys parenchyma with renal US, in children with TSC presenting urological symptoms, in particular micturitional disorders. References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11045f2.jpg] [pe11045f1.jpg] |
| |||||||||

{kind=link}
{kind=link}