 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 36, No. 1, Feb, 2004, pp. 10-14 Educational Forum AntiTNF-a strategy: Present status of this therapeutic paradigm J. Singh, A. Suruchi Department of Pharmacology, PGIMS, Rohtak - 124001,
India.
Received: 10.2.2003
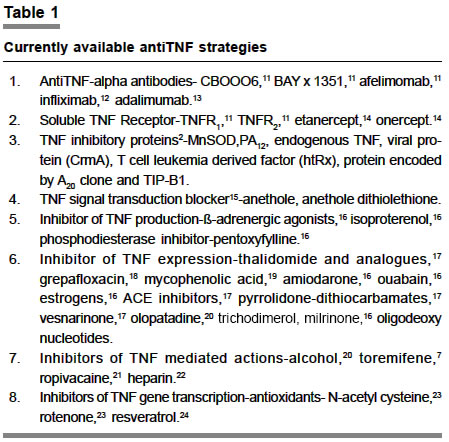
Code Number: ph03004 Abstract Tumor necrosis factor-alpha (TNF-a), a proinflammatory cytokine is involved in the pathophysiology of a number of disorders including Crohn's disease, rheumatoid arthritis, ankylosing spondylitis and psoriatic arthritis. AntiTNF-a strategies target this pathogenic element to provide clinical benefit. The various strategies are in preliminary stage of experimentation and much remains to be elucidated before these are applied clinically. Though antiTNF-a therapy is currently approved only for rheumatoid arthritis and Crohn's disease, the future of this therapeutic paradigm holds much promise. The number of official indications for strategies against this biologic agent are likely to increase to include congestive heart failure, psoriasis, asthma, septic shock, stroke and malignancy. This will make it a truly broad spectrum therapeutic weapon currently available to us. Key Words: AntiTNF-a therapy, etanercept, infliximab, tumor necrosis factor. Introduction Tumor necrosis factor-alpha (TNF-a) is a multi-functional cytokine with important role in immune response, inflammation and response to injury.1 TNF family is primarily involved in regulation of cell proliferation and apoptosis.1 TNF-a has also been shown to have an important role in cell death through a variety of mechanisms including second messenger pathways, arachidonate metabolism, protein kinase, oxygen free radicals, nitric oxide, transcription of a variety of cytotoxic genes, regulation of nuclear regulatory factors, ADP-ribosylation and potentially DNA fragmentation.1 TNF regulates expression of a variety of peptide regulatory factors including IL-1, IL-6, platelet derived growth factor, transforming growth factors-ß as well as a group of eicosanoids and hormones including platelet activating factors and adrenaline.1 It is now well recognized that TNF-a participates in the pathophysiology of various diseases/conditions including diabetes, multiple sclerosis, autoimmune diseases, cachexia, parasitic infections, AIDS,2 asthma,3 stroke,4 rheumatoid arthritis (RA),5 Crohn's disease,6 neurodegenerative disorders and malignancy.7 However, the role of TNF-a in the pathogenesis of malignancies remains controversial. Indeed, recent studies have demonstrated a causative role for TNF-a in a group of diseases including septic shock,8 pre-eclampsia,9 hemolytic uremic syndrome, allograft rejection, regional enteritis, and congestive heart failure.10 This review describes the role of TNF-a antagonists as a potential therapeutic weapon in various clinical conditions. Clinical strategies for antiTNF-a therapy AntiTNF strategies are aimed at blocking activity of TNF-a either through antiTNF-a antibody or administration of soluble TNF receptor to mop up circulating TNF-a. In addition to these, some proteins, TNF secretion/production inhibitors and expression inhibitors are also available11-24 (Table 1). AntiTNF-a therapy for rheumatoid arthritis TNF-a increases in rheumatoid joints and has a potential role in the establishment of rheumatoid synovitis and joint destruction.5 The use of TNF-a antagonists has taught us that selective targetting of a pathogenic element can provide substantial benefit, setting a new therapeutic standard for RA.5 AntiTNF-a therapy induces a rapid improvement in multiple clinical assessment of disease activity including morning stiffness, pain score, Ritchre articular index and swollen joint count. The clinical benefits are associated with an improvement in some serological parameters and histological features of the synovium.25 Several controlled clinical trials have clearly demonstrated short and middle term efficacy and safety profile of antiTNF-a therapy26 and they will soon become available worldwide. Infliximab and etanercept have been approved in US and Europe for treating RA.27 A multicentric double blind placebo controlled phase III clinical trial on 428 patients with active RA has shown that infliximab (3 mg/kg, every 4-8 weeks or 15 mg/week) + methotrexate for 3 weeks was more efficacious than methotrexate alone in patients with active RA not previously responding to methotrexate.28 However, some questions remain unresolved concerning their place in the general therapeutic strategy against RA, due to uncertainties of their use in the long run. If clinical efficacy is sustained and the safety profile remains benign over long term, TNF-a antagonists may replace methotrexate as a gold standard and become the agent of choice for combination therapy in RA. Further studies are needed to clarify their ultimate position in the therapeutic algorithm. Ankylosing spondylitis has also been successfully treated with infliximab.29,30 Similarly antiTNF strategies are being targeted at chronic inflammatory arthritides,12 such as psoriatic arthritis, sarcoidosis arthritis, idiopathic juvenile arthritis and spondyloarthropathy. AntiTNF-a therapy in Crohn's disease TNF is considered to be a crucial mediator of Crohn's disease (CD). Inflammatory cells of gastrointestinal lesions produce TNF and its concentration is increased in serum, tissue and stool. Present et al31 demonstrated that single i.v. infusion of infliximab (10 mg/kg) decreased the CD activity index score with improvement in colonoscopic evaluation. Infliximab has been found to be very effective in the treatment of fistula in patients with CD.31 Similar results have been reported in a controlled trial with etanercept.32 AntiTNF-a therapy in diabetes There is complex relationship between TNF-a and diabetic complications. TNF-a related apoptosis inducing ligand (TRAIL) is involved in ß cell damage leading to type I diabetes, causes insulin resistance, interferes with insulin signaling and influence the formation of atherosclerotic vascular lesions in diabetic patients.33 Increased TNF-a levels in patients with diabetes has been demonstrated and determination of TNF-a levels might offer a diagnostic tool to determine patients at high risk.34 Based on the available data, it can be inferred that antiTNF-a therapy may be beneficial in reducing the complications of diabetes, though no reports are available so far demonstrating them as potential therapeutic candidate. AntiTNF-a therapy in congestive heart failure TNF-a and other cytokines have been shown to be elevated in patients with end stage heart failure, heart failure due to myocarditis and ischemic and idiopathic dilated cardiomyopathy (CMP).10 TNF-a exerts negative inotropic effect, recapitulates cellular and biochemical abnormalities that characterise the failing human heart, uncouples ß-adrenergic receptors from adenylate cyclase, activates metalloproteinases and provokes a hypertrophic growth response in cardiac myocytes.10 TNF-a expression/production inhibitors have been shown to possess therapeutic utility in the management of patients with CHF. For an antiTNF-a drug to be useful in heart failure, it should not only be highly effective in reducing TNF-a levels but should also have other positive actions and should be orally active and cheap. As yet, no drug fits this description. Davey and Ashrafian17 demonstrated the therapeutic benefits of thalidomide and its derivatives in management of advanced heart failure. Recently, recombinant soluble TNF-a protein (S TNFR2) have been shown to be safe and capable of reducing raised levels of TNF-a-concomitantly lessening the severity of heart failure in patients with NYHA class III CHF.35 Intravenous infusion of etanercept increased exercise tolerance, ejection fraction and reported life score.35 Despite beneficial effects with antiTNF-a therapy, both hypertrophy and fibrosis persist suggesting early but not late therapy, using anticytokine approaches might benefit patients with CHF. demonstrated beneficial effect of grepafloxacin (a new fluoroquinolone) in controlling chronic airway inflammatory disease via expression of inhibitory TNF-a induced IL-8 mRNA. Therefore, an inhibitory effect of antiTNF-a therapy on IL-8 production may apply to the treatment of chronic airway inflammatory disease. However, further investigations are needed to clarify this point. Treatment directed specifically at a reduction in TNF-a activity may be useful as a glucocorticoid sparing asthma therapy. AntiTNF-a therapy may also be effective in the treatment of certain allergic conditions including Jarisch-Herxheimer reaction.37 It is well established that recruitment of neutrophils and eosinophils associated with allergic condition is mediated via TNF-a.1 AntiTNF-a therapy in sepsis and shock TNF-a is a principal mediator in the pathophysiology of septicemia and elevated levels of TNF-a have been reported in patients with sepsis.8,11 Attempts to block TNF-a activity have been associated with improved survival in animal models of sepsis and shock.11 In human studies, 7.5 mg/kg, TNF-a monoclonal antibody provided a significant reduction in mortality 30 days after infusion.38 Antibodies have been found effective in reducing early morbidity and mortality but no reduction in 28 days mortality. Drugs that modify TNF in vivo may be an useful component of future management of sepsis either as monotherapy or as part of combined strategy of immunomodulators. Afelimomab has been tested in 7300 patients with septic shock and found to be efficacious and well tolerated.11 However, in sepsis, findings have not been so convincing. The use of antiTNF-a in the wrong patient or at the wrong time may do more harm than good. Although antiTNF-a such as afelimomab may yet prove valuable in treatment of carefully selected patients with severe sepsis, further work is needed to clarify the selection criteria of patients who will be benefited the most. AntiTNF-a therapy in malignancy TNF-a promotes cell growth, differentiation, tissue remodeling and tumorigenesis.16 On the other hand, recombinant TNF-a is reported to be selectively cytotoxic for some tumor cell lines and causes necrosis of certain murine tumors. Although TNF promotes angiogenesis,7 antiangiogenic effect on tumor microvasculature has also been reported.39 Therefore, the role of TNF-a in the pathogenesis of malignancies remains controversial. However, direct relationship between the level of TNF expression and tumor grades in ovarian cancer has been reported.40 Naylor et al40 demonstrated the therapeutic potential of antiTNF therapy in human epithelial ovarian cancer. Monoclonal antibodies against TNF-a have proved successful in ameliorating cachexia of cancer.16 Skin tumors such as basal cell carcinoma have been shown to be associated with TNF microsatellites.41 Although a few preliminary studies have demonstrated beneficial effect of antiTNF therapy in ovarian and colorectal cancers, much remains to be elucidated as far as exact place of anti-TNF therapy in cancer treatment is concerned. The TRAIL offers great promise in cancer therapy. Soluble recombinant versions of the TRAIL molecule have exhibited specific tumoricidal activity against a variety of tumors alone, or in combination with other cancer treatments.42 The TRAIL effector pathway appears to be a vital component of immunosurveillance of tumor cells, stimulating more hope that manipulating TRAIL activity is a natural path to improved cancer immunotherapy. Lin et al43 found that breast cancer cell lines resistant to chemotherapy or to recombinant TRAIL protein are susceptible to TRAIL gene therapy suggesting that combination of TRAIL gene therapy and chemotherapy is effective in the treatment of metastatic diseases. TRAIL therapy is now being tried in a wide variety of neoplasms. AntiTNF therapy in dermatology AntiTNF-a arsenal is an exciting addition to dermatologic therapy. New molecules are expected to enrich the antiTNF-a arsenal. A recently reported double blind trail by Chaudhari et al44 showed a greater than 75% improvement in psoriasis, area and severity index score at week 10, in 9 out of 11 (82%) patients receiving infliximab 5 mg/kg at weeks 0, 2 and 6, indicating efficacy and rapidity of onset of therapeutic effect similar to cyclosporine. Etanercept has been shown to possess good efficacy in moderate to severe psoriasis.45 Encouraging sporadic results suggest potential indications in Behcets disease, bullous dermatitis, neutrophilic dermatitis, toxic epidermal necrolysis, systemic vasculitis, pyoderma gangrenosum46 and pustular dermatitis.47 A recent report by Warnnissorn et al48 has shown involvement of TRAIL in atopic dermatitis. AntiTNF-a therapy in other conditions Beneficial role of antiTNF-a therapy has also been demonstrated in various clinical conditions such as alcoholic hepatitis,49 cerebral malaria,50 hemolytic uremic syndrome,16 preeclampsia,9 allograft rejection,16 otitis media,51 snakebite,52 erythema nodosum and other granulomatous diseases.53 Potential new indications include, adult Still's disease, myelodysplastic syndromes,54 graft versus host disease54 uveitis,54 dermatomyositis and polymyositis.55 Adverse effects Early experience with antiTNF-a therapy has identified 7 types of adverse effects that seem to be of particular concern (a) infection including sepsis and tuberculosis (b) malignancies such as lymphoma (c) hematological disorders such as anemia and pancytopenia (d) demyelinating disorders and neuropathy (e) exacerbation of CHF (f) production of autoantibodies and autoimmune responses (immunosuppression) (g) infusion related problems (as hypersensitivity pain, erythema, localized rash and hemorrhage at injection site. Immunocompromised and geriatric patients are at increased risk of severe side effects.29,30 Blockers of TNF have been associated with occurrence of cutaneous vasculitis also.56 Therefore, antiTNF-a therapy can be labeled as a double edged sword. Conclusion AntiTNF-a therapy is currently approved for the treatment of rheumatoid arthritis and Crohn's disease. It is clear that the number of official indications for antiTNF-a therapy will increase to include congestive heart failure, psoriasis, malignancy and asthma. However, the compound has already gained a unique niche as a biologic therapy. Exciting pilot studies are being done on TNF-a antibodies to find their utility in clinical conditions such as septic shock, diabetes, stroke and multiple sclerosis. Finally, it may be anticipated that new indications will be discovered for these agents-making it a truly broad-spectrum therapeutic weapon currently available. References
Copyright 2004 - Medknow Publications on behalf of the Indian Pharmacological Society. Free, full-text articles also available from http://www.ijp-online.com The following images related to this document are available:Photo images[ph04004t1.jpg] |
| |||||||||

{kind=link}