 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 36, No. 1, Feb, 2004, pp. 20-24 Reversal of phenytoin-induced impairment of spontaneous alternation by piracetam in mice: Involvement of cholinergic system M. Shahid, K. K. Pillai, D. Vohora Department of Pharmacology,
Faculty of Pharmacy, Jamia Hamdard, New Delhi - 110062, India.
Received: 15.11.2002
Code Number: ph04006 Abstract Objective: To study the effect of the combined treatment
of phenytoin and piracetam on seizure control, cognitive and motor functions
in mice.
KEY WORDS: Acetylcholinesterase, cognitive functions, diphenylhydantoin, piracetam. Introduction Phenytoin (PHT) is one of the low-cost and widely prescribed antiepileptic drugs (AED) known to cause cognitive impairment. Many studies have investigated the effect of PHT on learning, memory and psychomotor functions. Both acute and chronic administration of PHT has been shown to significantly impair learning and memory.1-3 For an optimum antiepileptic therapy, it is desirable to have complete seizure control without interfering cognitive effects. A combination of antiepileptic drugs (AEDs) with known nootropic agents appears to be a promising research area for desirable seizure control with minimal/no memory deficit. A better approach would be to use an agent that not only corrects the cognitive disturbances but also provides seizure protection. In this regard, one of the promising agents is piracetam (PIM). PIM (2-oxo-1-pyrolidone acetamide)a nootropichas been shown to be an effective antimyoclonic agent.4-6 It has been shown to have a specific antiamnesic activity in many experimental paradigms.7-9 In addition, it has demonstrated a protective effect against pentylenetetrazol (PTZ) kindling-induced neuronal loss and learning deficit.10 However, it lacks anticonvulsant activity in the MES model.7 Convincing neuroprotective functions have also been shown experimentally.11,12 Thus it would be worthwhile to assess the use of PIM along with PHT on seizure and cognitive functions. The central cholinergic system plays an important role in learning and memory.13-15 PHT is known to reduce hippocampal ACh concentration.2,16,17 In view of this we also studied the effect of this combination on the brain cholinergic system. Since the majority of AEDs including PHT are known to impair motor performance, the study also evaluated this combination on motor function. Material and Methods Animals Swiss albino mice of either sex (24-34 g), supplied by the Central Animal House Facility of Jamia Hamdard, New Delhi (Registration no. 173/CPCSEA) were used. All animals were housed in cages in groups of 10, at 23-300C with a natural light-dark cycle. They had free access to standard pellet diet (Amrut Laboratory rat and mice feed, Navmaharashtra Chakan oil mills Ltd., Pune) and tap water. The study has been approved by the Ethics committee, CPCSEA (project no. 64, Nov. 2001). Ethical norms were strictly followed during all experimental procedures. Drugs and dosing schedules The following drugs were used: Phenytoin (`Dilantin' suspension, Parke Davis) was given p.o. in a volume of 10 ml/ kg body weight in doses of 8, 12 and 22 mg/kg body weight 2 h prior to each observation. Piracetam (`Nootropil' syrup, UCB) was given p.o. in a volume of 10 ml/kg body weight in doses of 125, 250 and 500 mg/kg body weight 1 h prior to each experiment. Control groups were given distilled water in a volume of 10 ml/kg body weight. Chronic studies were done for 21 days. All observations were made on day 21 after 2 h of phenytoin and 1 h of piracetam administration. In chronic studies, drugs were administered between 10-12 A.M. Increasing Current Electroshock Seizures (ICES) The ICES as proposed by Kitano et al18 and modified by Marwah et al19 was used to evaluate the anticonvulsant effect of the drugs. To start with a current of 2 mA electroshock to each mouse via ear electrodes as a single train of pulses (for 0.2 sec) was given with linearly increasing intensity of 2 mA / 2 sec using an electroconvulsometer (INCO, Ambala, India). The current at which tonic Hind Limb Extension (HLE) occurred was recorded as the seizure threshold current (STC). When no tonic HLE was observed by a current of 30 mA, electroshock was terminated. Spontaneous Alteral Behavior (SAB) on a plus maze Rodents have a natural tendency to alternate. An amnesic drug impairs this behavior and vice versa with nootropics. Hence, an increase in alternation implies improved cognition and vice versa. Cognitive functions were assessed using a plus maze proposed by Itoh et al20 and SAB was noted following the method of Ragozzino et al.21 The maze (height50 cm) was constructed of wood, painted gray and contained a central platform (8 X 8 cm) from which radiated four symmetrical arms (23.5 X 8 cm) with 10 cm walls. After being placed in the central platform, mice were allowed to traverse the maze freely. The number and sequence of entries were recorded during an observation period of 6 min. An alternation was defined as entry into four different arms on overlapping quintuple sets. Five consecutive arms choices within the total set of arm choices make up a quintuple set, e.g. a quintuple set consisting of arms choices A, B, A, C, B was not considered an alternation. Using this procedure percentage alternation was calculated as follows:
The number of arm entries was also recorded separately to determine the motor influence on the observed effects. Rolling roller apparatus This method as devised and proposed by Dunham et al22was used to screen the neurological deficit caused by the drugs. The speed selector was set so that the roller made 5 revolutions/minute. The animals were placed on the roller for one minute as a testing time. A normal animal can maintain its equilibrium throughout the period. Neurological deficit was indicated by the inability of the animal to remain on the roller for a one-minute test period.
Estimation of brain acetylcholinesterase (AChE) activity The whole brain AChE activity was measured using the Ellman et al method.23 This was measured on the basis of the formation of yellow color due to the reaction of thiocholine with dithiobisnitrobenzoate ions. The rate of formation of thiocholine from acetylcholine iodide in the presence of tissue cholinesterase was measured using a spectrophotometer. The sample was first treated with 5,5'-dithionitrobenzoic acid (DTNB) and the optical density(OD) of the yellow color compound formed during the reaction at 412 nm every minute for a period of three minutes was measured. Protein estimation was done using Folin's method. AChE activity was calculated using the following formula: Statistical analysis The data were expressed as mean+SEM. The normally distributed data were subjected to one-way ANOVA followed by Dunnett's test. Kruskal Wallis one-way ANOVA followed by multiple range test was used for the analysis of non-normally distributed data. P values <0.05 were considered significant.
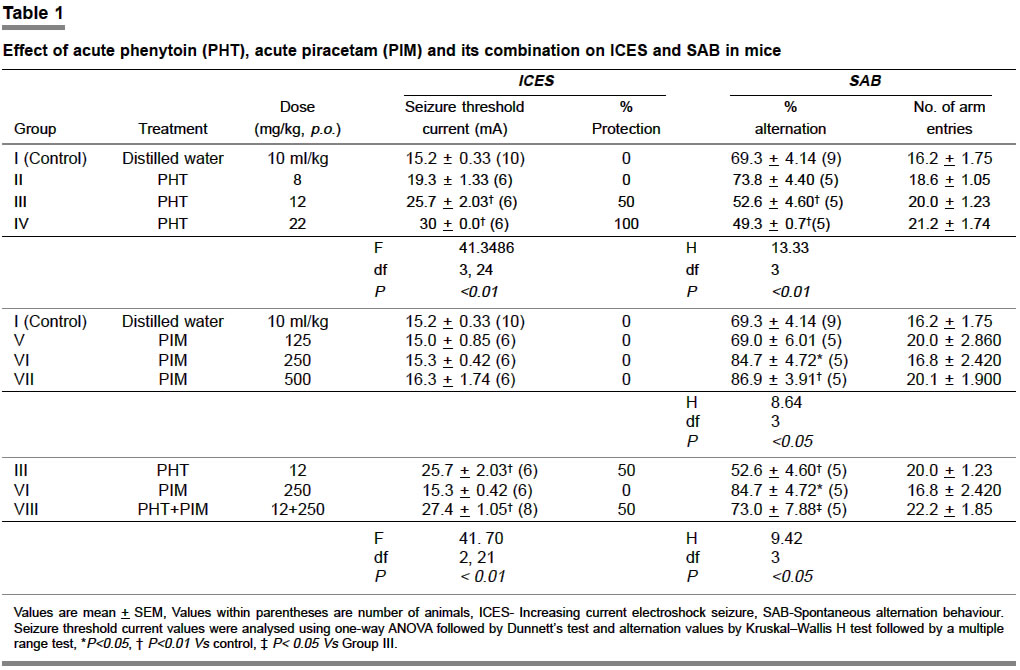
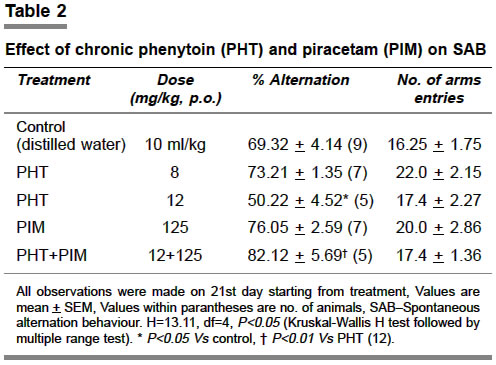
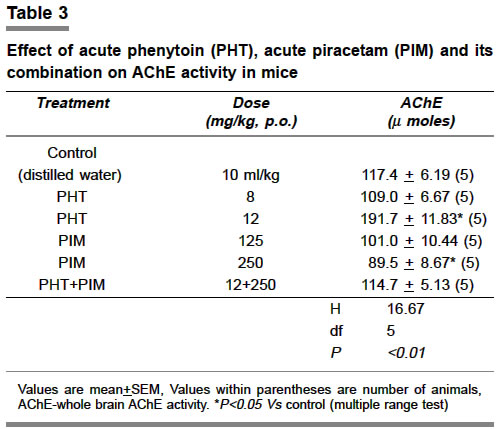
Results Increasing current electroshock seizures (ICES) Acute studies: PHT (22 mg/kg, p.o.) showed 100% protection against ICES as evidenced by a complete abolition of HLE. PHT (12 mg/kg, p.o.) produced 50% protection while a low dose of PHT (8 mg/kg, p.o.) afforded 0% protection (Table 1). PIM, at memory improving doses derived from Table 1 was found ineffective on ICES (Table 1). Spontaneous alternation behavior Acute studies The administration of PHT (12-22 mg/kg, p.o.), significantly reduced percentage alternation on plus maze, which accounts for the adverse effect on cognitive function. A lower dose (8 mg/kg, p.o.) did not elicit such an effect (Table 1). PIM (250-500 mg/kg, p.o.) showed significant elevation of percentage alternation while a dose of 125 mg/kg was ineffective (Table 1). Combined treatment with PHT (12 mg/kg, p.o.) and PIM (250 mg/kg) showed effects similar to the control group i.e. no deteriorating effect on memory without altering any effect on ICES (Table 1). Chronic studies PHT (12 mg/kg, p.o. X 21 days) caused a significant reduction in the percentage alternation i.e. markedly impaired memory. Combination of PIM (125 mg/kg, p.o. X 21 days) with PHT (125 mg/kg, p.o. X 21 days) reversed such an impairment (Table 2). Rolling roller apparatus: No dose of PHT and PIM in both acute and chronic studies, as well as in combination, produced any motor deficit. Whole brain AChE activity The whole brain AChE activity with PHT (8 mg/kg, p.o.) did not differ from the control. However, PHT (12 mg/kg, p.o.) demonstrated a significant rise in AChE activity as compared to control. PIM at a dose of 125 mg/kg, p.o. did not alter brain AChE activity significantly but at a dose of 250 mg/kg, p.o. lowered AChE levels significantly. A combination of PHT (12 mg/kg, p.o.) and PIM (250 mg/kg, p.o.) exhibited AChE levels similar to control (Table 3). Discussion The results of the present study show that PHT in doses 12-22 mg/kg, p.o., adversely affected the cognitive function in both acute and chronic studies. These doses were indeed found to be ED50 and ED100 against ICES. This result is in agreement with the previous studies of PHT on cognitive functions.1-3 PIM, a well-known nootropic agent7-9 as well as an antimyoclonic agent4-6 exhibited significant nootropic effect on spontaneous alternation behavior, a model specific for measuring spatial memory in rodents. At the nootropic doses used, it was found to be ineffective against ICES thus consistent with the earlier reports on the MES model.7 Higher doses of PIM, however, were found to have significant antiepileptic effect against ICES (data not shown). The present study was based on the assumption that coadministration of PIM with clinically used AED might be useful in reducing some of the cognitive adverse effects of antiepileptic therapy. Our study showed that PIM, when coadministered with PHT, significantly reversed PHTinduced cognitive impairment without altering the efficacy of PHT against ICES. In the chronic study, PIM at lower dose of 125 mg/kg enhanced the percentage alternation but it was not statistically significant. This dose, however, could reverse the PHT-induced impairment of SAB. This is in agreement with another report where PIM was shown to prevent PTZ kindling-induced neuronal loss and learning deficits.10 To study the effect of motor influences on observed effects, the rolling roller apparatus was used but PIM alone, as well as in combination with PHT, did not exhibit any significant effect on motor functions. Further, the number of arm entries remained unaffected in SAB, thus ruling out the involvement of motor functions in the observed cognitive effects. The precise mechanism by which PIM exerts its nootropic effect is not known. Multiple mechanisms have been suggested such as an enhancement of oxidative glycolysis,24 an effect on the Ca2+ channels25 and an effect on the cholinergic system.24 The latter is known to have an important role in the learning and memory processes. In our study, PHT, per se (12 mg/kg, p.o.) significantly elevated the `brain AChE activity'. PIM (250 mg/kg, p.o.) on the other hand significantly lowered this activity indicating the counteracting action of the two drugs on the cholinergic system. The impairing effects of PHT on learning and memory have been attributed to alternations in the cholinergic system.2,16,17 It has been reported that PHT lowers brain ACh levels.2,16,17 Our results on AChE are thus consistent with these reports. It is worth noting that PHT at 8 mg/kg, p.o., did not show an impairment and did not affect AChE levels. PIM is a member of the pyrrolidones group. Most of the pyrrolidones are known to influence cholinergic functions. ACh production and turnover are stimulated by most pyrrolidones but with varying actions at muscarinic and nicotinic receptors.8,11,24 In our study PIM reduced the AChE activity of the brain. But, more importantly, in this context, it is interesting to note that when coadministered with an effective dose of PHT, PIM significantly alleviated the PHT-induced sharp rise in total brain AChE level, indicating the counteracting action of PIM and PHT on the cholinergic system. To conclude, PIM when coadministered with therapeutic doses of PHT, significantly alleviated the adverse effects of PHT on cognitive function without compromising its antiepileptic efficacy, the effect possibly mediated by an action on the cholinergic system. However, clinical studies are required to explore the full potential of PIM in correcting PHT-induced cognitive deficits and finding a place in the current AED therapy. References
Copyright 2004 - Medknow Publications on behalf of the Indian Pharmacological Society. Free, full-text articles also available from http://www.ijp-online.com The following images related to this document are available:Photo images[ph04006t3.jpg] [ph04006t2.jpg] [ph04006t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}