 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 36, No. 1, Feb, 2004, pp. 29-33 Comparative bioavailability of three oral formulations of sustained release theophylline in healthy human subjects N. Parvez, T. Ahmed, T. Monif,* N. Saha,* P. L. Sharma Department of Pharmaceutical Medicine, Faculty of Pharmacy, Jamia
Hamdard, Hamdard University, New Delhi - 110062, India. *Department of Clinical
Pharmacology and Pharmacokinetics, Ranbaxy Research Laboratories, Gurgaon -
122001, India.
Received: 5.5.2003
Code Number: ph04008 Abstract Objective: To determine the bioequivalence of two marketed
test formulations (A, B) as compared to a reference formulation (R) of slow
release theophylline in healthy volunteers.
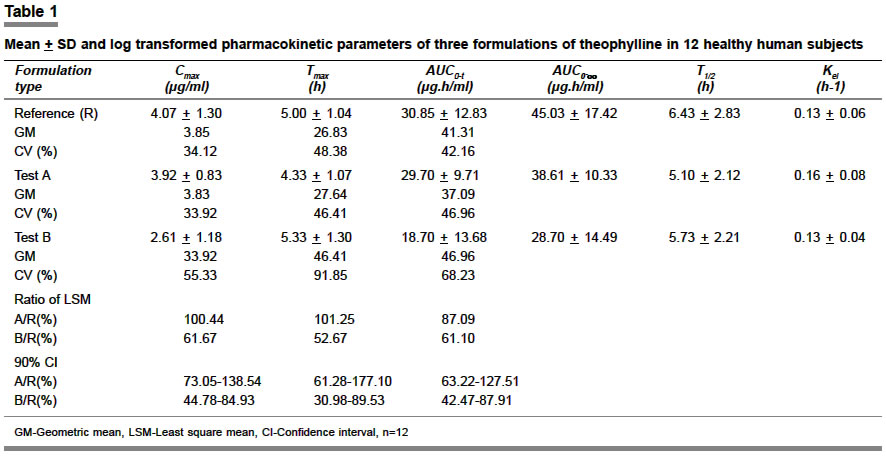
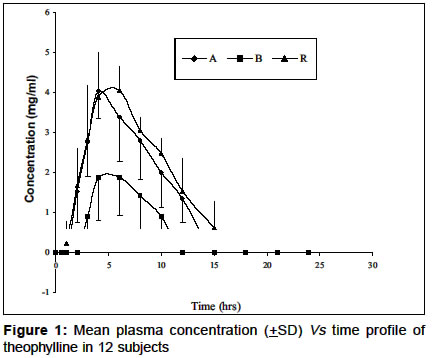
KEY WORDS: Bioequivalence, theophylline. Introduction Systemic drugs administered orally or parenterally must reach the general circulation in their pharmacologically active form to be distributed throughout the body and to exert therapeutic effect. The intensity of the therapeutic actions of many drugs correlate well with the concentration of the drug in the biological fluid.1 The rate of absorption is therapeutically important with single doses of drugs, especially in case of narrow therapeutic index drugs,2 where relatively small changes in the concentration can lead to marked changes in pharmacodynamic response. Theophylline is a narrow therapeutic index drug and exhibits dose-dependent pharmacokinetics.3 It is commonly used for the control and management of acute asthma and acute exacerbations of chronic obstructive lung disease.4 Although most of the available oral preparations are well tolerated, the desired plasma theophylline concentrations of 10-20 µg/ml are difficult to achieve.5 Theophylline is a drug with a short half-life, so rapid release theophylline preparations are required to be administered in multiple daily doses, which may lead to poor patient compliance and hence inadequate therapeutic response. In order to overcome these problems, sustained release (SR) preparations of theophylline have been developed and marketed. A number of sustained release preparations of the drug are commercially available on the Indian market. These slow release products are formulated in various ways that decrease the rate of disintegration and dissolution of the drug, thus affecting the bioavailability.6 The medical profession has realized the problem of wide variations in the therapeutic effectiveness of various brands of oral formulations containing the same active ingredient in equal amounts. Once patients are stabilized on one slow release preparation, they should not be changed to another product without retitration of dosage with careful monitoring of plasma theophylline levels, as it is a narrow therapeutic index drug to achieve optimum therapeutic levels with minimum toxicity.4 Most of the bioequivalence studies on which the claims of bioequivalence to innovator product do not use confidence intervals (CI). Determination of CI is a current regulatory requirement of DCGI (Drug Controller General of India) and also of FDA7 (http://www.fda.gov/gov/cder/guidance/index.htm; April, 2003) to document bioequivalence. Thus, the only way to verify these claims is to do a comparative bioequivalence study with the innovator drug formulation, using confidence intervals. Hence, the present study was undertaken to compare the bioavailability of three brands of 200 mg sustained release theophylline in healthy, adult, male, human subjects under fasting conditions. Materials and Methods Products evaluated Reference (R) Theostan CR-200 mg capsule manufactured by Sidmak Labs. Ltd.,Gujrat, Batch No. T-00600, Mfd. Nov. 2000, Exp. Oct. 2002. This was taken as reference as it was the first entrant in the Indian market. Test (T) (A) Phylobid 200 mg SR tablets manufactured by Tridoss India Ltd., Aurangabad, Batch No. 11026, Mfd. Dec. 2001, Exp. Nov. 2002. (B) Theobid 200 mg SR tablets manufactured by Osaka Pharma Ltd., Satara, Batch No. S10255, Mfd. Sep. 2001, Exp. Aug. 04. Study design The study was conducted as an open label, balanced, randomized, three-treatment, three-period, three-sequence single-dose crossover study in 12 healthy adult, male, human subjects, under fasting conditions, comparing the bioequivalence of the two test products (A, B) with the reference formulation (R). Each subject received one 200 mg theophylline formulation with 240 ml of drinking water after an overnight fast during each of the study day. The order of receiving the different treatments for each subject during the three periods of the study was determined according to SAS-generated randomization schedule. There was a washout period of seven days between each study period. Study subjects Twelve healthy, adult, male subjects participated in the study. The mean+SD age and weight of the subjects was 22.66+2.74 years (range 19-26) and 57.75+9.15 kg (range 46-76) respectively. All were in good health as evidenced by the medical histories, complete physical examination and routine laboratory tests performed within 28 days prior to the commencement of the study. None had history of any allergy to theophylline and related compounds. Subjects did not receive any medication during the two weeks period prior to the start of the study. They were instructed during screening not to take any prescription and OTC medications subsequently until the completion of the study. All the subjects abstained from any xanthine-containing food or beverages or alcoholic products for 48 h prior to dosing and throughout the sampling schedule during each period. Smokers and alcoholics were excluded from the study. Subjects were admitted and housed in the Clinical Pharmacology Unit from 12 h before dose and were discharged 24 h after dose during each period. A total of 42 blood samples (5 ml each) were collected pre dose and at 0.5, 1.0, 2, 3, 4, 6, 8, 10, 12, 15, 18, 21 and 24 h post dose through an indwelling cannula placed in a forearm vein during each period. After collection, the blood samples were centrifuged to separate the plasma. All plasma samples were stored at -700C until analysis. Ethical considerations The study was conducted at Ranbaxy Clinical Pharmacology Unit (Majeedia Hospital, New Delhi) according to a protocol approved by the Jamia Hamdard Institutional Review Board. This research was carried out in accordance with the clinical research guidelines defined in the U.S. 21 CFR part 312.20 and the principles enunciated in the Declaration of Helsinki (South Africa 1996). All the subjects provided written informed consent before entering the study. Bioanalytical method Theophylline was assayed by high performance liquid chromatography (HPLC) according to the method described in a previous study,8 but with some modifications. The sample preparation process was accomplished by protein precipitation using acetonitrile. The supernatant was chromatographed on an ODS spherisorb column (25 cm X 4.6 mm ID) with a particle size of 10 µm using the mobile phase consisting of anhydrous sodium acetate buffer and acetonitrile (92:8 v/v). The pH of the mobile phase was adjusted to 5.0 with 10% glacial acetic acid. The analysis was carried out at a wavelength of 273 nm. Signals from the detector were captured in a computer, and processed by using Millennium 32 software. The method was validated by following international guidelines.9 The assay was found to be selective, accurate and precise with a linear range of 0.625 µg/ml to 20.0 µg/ml. The within batch accuracy ranged from 92.0 to 105.5% while the total accuracy of the assay ranged from 94.32% to 101.96%. The total precision of the method ranges from 5.51 to 8.52% while the within batch precision of the method ranges from 1.7 to 13.25%. The stability of the spiked plasma samples was determined during two freeze thaw cycles. Replicate numbers of low and high quality control samples were analyzed for the first and second freeze thaw cycles. The stability in the first and second freeze thaw cycles was 93.22 to 108.7% and 96.06 to 99.33% respectively. Hence theophylline was stable for two freeze thaw cycles. Pharmacokinetic analysis The various pharmacokinetic parameters were calculated using WinNonlin software Version 1.5.10 The maximum plasma concentration (Cmax) and the time to reach Cmax (Tmax) were determined by visual inspection of the individual plasma-concentration time profiles. Terminal elimination rate constant (Kel) was calculated from a semi-log plot of the plasma concentration versus time curve. This parameter was calculated by linear least square regression analysis using the last three (or more) non-zero plasma concentrations. The terminal half-life was calculated by the formula 0.693/Kel. The area under the concentration-time curve (AUC) was calculated by the linear trapezoidal method. Statistical analysis All statistical analyses were carried out using SAS software version 6.12 (SAS Institute Inc. Cary NC, USA). The AUC0-t, AUC0-¥ and Cmax values were log converted before analysis. Ratio of mean (in percentage) was calculated using the least square mean (LSM) for log transformed AUC0-t, AUC0-¥ and Cmax values. Ratios of mean were expressed as a percentage of the LSM for the respective treatment comparisons. The 90% CI of AUC0-t, AUC0-¥ and Cmax for the ratio of test and reference was determined to assess the bioequivalence between different products using the equivalence interval of 0.80 and 1.25. The USFDA7 recommend the limit of 80-125% for AUC and 90-111% for Cmax for narrow therapeutic index (NTI) drugs. The Indian regulatory guidelines also recommend the same limits for NTI drugs. The intrasubject variability was determined using WinNonlin software Version 1.510 for the pharmacokinetic parameters AUC0-t, AUC0-¥ and Cmax. Analysis of variance (ANOVA) was also performed and a statistically significant difference was considered at P<0.05. Results There were no significant protocol deviations and all the 12 subjects completed the study. The various pharmacokinetic parameters after the administration of theophylline 200 mg sustained release formulation manufactured by different pharmaceutical companies are shown in Table 1. The mean plasma theophylline concentration versus time profile for all the treatments is shown in Figure 1. There was no period, sequence and formulation effect as indicated by the P values for different treatments. The T/R (test/reference) ratios for the pharmacokinetic parameters AUC0-t, AUC0-¥ and Cmax were satisfactory for product A (Phylobid) and were 100.44%, 104.18%, and 89.78% respectively. For product B (Theobid) the ratios for these parameters were 61.67%, 52.67%, and 61.10%. However, when 90% CI was applied for the log-transformed pharmacokinetic parameters, the upper and lower confidence limits for both the products fell outside the prescribed limits of bioequivalence for narrow therapeutic index drugs i.e. 90-111% for log-transformed data for Cmax and AUC. The intrasubject variability (ISV) for the log-transformed pharmacokinetic parameters was quite high (For Test A: ISV for Cmax, AUC0-t, and AUC0-¥ 33.78, 22.68 and 14.10; Test B: 53.14, 28.63 and 15.79 respectively). Discussion This study demonstrates that both the test products of theophylline were not bioequivalent to the reference product. The T/R ratios of product A were quite close to the prescribed limits of bioequivalence (95%-105%). The bioavailability of product B was very poor indeed. The desired ratio of AUC0-t/AUC0-¥ (80% or more) is low in this study, this could be due to the fact that in present study the choice of limit of quantitation (LOQ) is high and should have been preferably much lower. In a study carried out by Bhandari,11 the bioequivalence of two brands of SR theophylline was studied in 12 subjects. A single dose of 400 mg SR theophylline was administered. The Cmax of the reference formulation was 8.56+0.50 µg/ml at 11.00+1.28 h. The Cmax of the test formulation was 9.95+0.68 µg/ml at 10.83+1.28 h. The AUC0-24 was 140.57+8.19 µg.h/ml for the reference formulation and for the test formulation it was 165.80+9.83 µg.h/ml. The AUC0-¥ for the reference formulation was 483.65+193.20 µg.h/ml and for the test formulation it was 374.77+66.54 µg.h/ml respectively. They concluded that both the preparations resulted in comparable mean plasma theophylline levels throughout 24 h and were bioequivalent with respect to the T/R ratios. However, the confidence intervals, the acid test for demonstrating bioequivalence12 were not applied. Another crucial drawback of this study was that only one time point was sampled after the Cmax and adequate sampling (at least 3 blood samples) was not done during the elimination phase of the drug, but surprisingly all the pharmacokinetic parameters i.e. AUC0-¥ Cmax, t1/2 and Kel were calculated. In an earlier bioavailability study carried out on 8 healthy adult volunteers, three solid and one (reference) liquid theophylline products were studied.13 In yet another study14 conducted on 12 healthy human volunteers, two SR theophylline preparations were studied. In both these studies, confidence intervals were not used to document bioequivalence. It is thus clear that most of the bioequivalence studies carried out on theophylline did not use confidence intervals while concluding bioequivalence. Theophylline being a narrow therapeutic index drug, it is legally incumbent on the manufacturers to ensure the quality of the marketed formulations, since a small change in the systemic concentrations may lead to a marked change in the pharmacodynamic response, with undesirable therapeutic consequences. Thus, asthmatic patients whose therapeutic response to theophylline, in approved doses, is sub-optimal may not necessarily be drug-resistant. The sub-optimal response may be due to achievement of sub-therapeutic plasma levels due to poor oral bioavailability of some of the marketed theophylline formulations. In the present study, the bioavailability of the test product A was 89.78% with respect to the reference and the bioavailability of the test product B was 61.1 % with respect to the reference. So the product A i.e. Phylobid has almost comparable bioavailability to the reference product i.e. Theostan CR and can safely be substituted in case of non-availability of the reference product, but the same cannot be recommended for the product B i.e. Theobid. The results obtained in this study indicate that various formulations of theophylline (a narrow therapeutic index drug) marketed by different pharmaceutical companies in India may differ significantly in their bioavailability. The physicians prescribing these products, unsuspectingly presume that the quality of different formulations if not exactly the same, is nearly the same. The resultant sub-therapeutic response in many patients may, in fact be due to significantly poor bioavailability from the particular formulation prescribed. Since most practicing physicians in India do not have access to therapeutic drug monitoring, it is the legal as well as moral duty of the manufacturers of marketed formulation of theophylline to ensure bioequivalence with the innovator's formulation, not only at the time of obtaining Regulatory Marketing Approval but also for subsequent batches of the formulations marketed by them over the years. Acknowledgements This research was supported by a grant provided by Ranbaxy Research Laboratories, Gurgaon, India. The authors would like to thank the staff of the Ranbaxy Clinical Pharmacology Unit and Department of Clinical Pharmacology and Pharmacokinetics for their support to conduct this study and analysis of clinical samples. The authors are also grateful to Late Janab Hakeem Abdul Hameed for providing excellent facilities at the university. References
Copyright 2004 - Medknow Publications on behalf of the Indian Pharmacological Society. Free, full-text articles also available from http://www.ijp-online.com The following images related to this document are available:Photo images[ph04008t1.jpg] [ph04008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}