 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
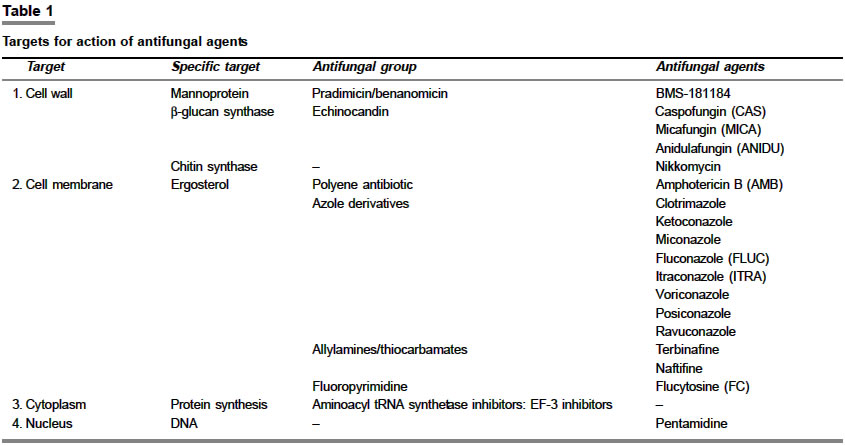
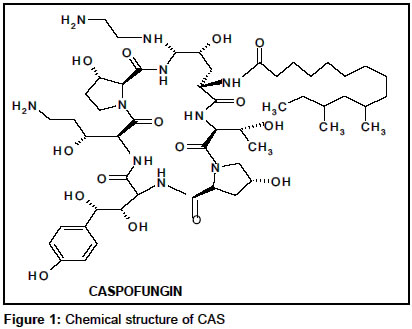
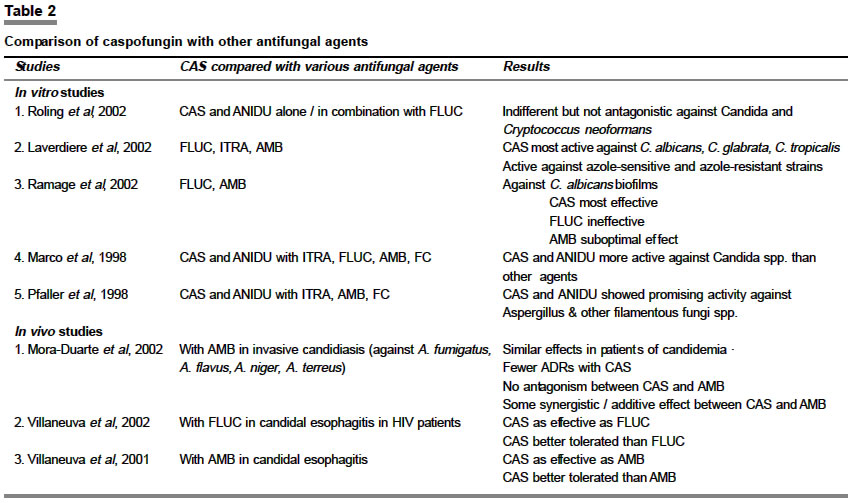
Indian Journal of Pharmacology, Vol. 36, No. 2, April, 2004, pp. 65-71 Education Forum Echinocandins: A promising new antifungal group Randhawa GK, Sharma G Department of Pharmacology, Government Medical College, Amritsar, Punjab Code Number: ph04027 ABSTRACT Echinocandins are a new option for fungal infections. They are fungicidal and less toxic to the host by virtue of their novel mechanism of action. They are b-1, 3-glucan synthase inhibitors. FDA, USA has approved caspofungin for treatment of invasive aspergillosis in patients who fail to respond or are unable to tolerate other antifungals. Two other agents are in phase III clinical trials – micafungin and anidulafungin. Caspofungin among echinocandins has been studied vastly and offers apparent exciting advantages of a broad spectrum of activity including strains of fungi resistant to other antifungal agents, tolerability profile, with no nephrotoxicity and hepatotoxicity as compared to azole and macrolide antifungals. It may be effective in AIDS-related candidal esophagitis, oropharyngeal candidiasis, fungal pneumonia and nonmeningeal coccidioidomycosis. Clinical trials are required to ascertain their safety in special groups—pediatric, pregnant and nursing mothers. Echinocandins provide an exciting option for combination therapy with other antifungals in fulminant fungal infections.INTRODUCTION The incidence of severe, invasive and opportunistic fungal infections in immunocompromised patients like those treated with immunosuppressive drugs, intensive chemotherapy, in organ transplant recipients, AIDS patients and very low birth weight infants, is increasing at an alarming rate.[1],[2] Mortality among infected patients may be as high as 75-100%, presenting an enormous challenge for healthcare providers.[3] The most common fungal pathogens are Candida and Aspergillus spp.[4] Recent epidemiological trends indicate a shift towards infections with Aspergillus spp., non-albicans Candida spp. and previously uncommon fungi with decreased sensitivity to antifungal agents.[1],[5],[6],[7] There has been a dramatic increase in the armamentarium for fungal infections in the past one decade. Antifungal drugs for serious infections are either fungistatic (fluconazole, itraconazole, i.e. azoles) and vulnerable to resistance or fungicidal (amphotericin B - polyene macrolide) but toxic to the host. A newer option, echinocandins are fungicidal and are less toxic to the host by virtue of their novel mechanism of action. Antifungal agents with different mechanisms of action and different adverse effect profiles have opened up new avenues for combination therapy to combat potentially life-threatening diseases. Targets for action of antifungal agents are given in [Table - 1] . Cell wall-acting agents are a new class of antifungals with a novel mechanism of action and are inherently selective and fungicidal in nature. Three classes of such compounds, targeted respectively to b-1, 3-glucan synthase (echinocandins- a derivative of pneumocandin B0), chitin synthase (nikkomycins) and mannoproteins (pradimicins/benanomicins), were explored for clinical development. Amongst them, echinocandins (caspofungin acetate, micafungin and anidulafungin) have emerged as potentially clinically useful entities.[8] Diagnostic procedures Evolving new diagnostic procedures for fungal infections would be helpful in early diagnosis and prevention of disease, hence better and timely management of fungal infections with decreased mortality. The clinical diagnosis is difficult based upon symptoms, which are non-specific and similar to those of bacterial and viral infections. Previously used methods such as direct microscopic examination of clinical samples and serological tests have limited success. Improvements in diagnostic procedures like high-resolution computed tomography,[9] polymerase chain reaction[10] and enzyme-linked immuno-sorbent assay[11] for invasive pulmonary aspergillosis have limited definitive prognostic value. A standardized method for testing the in vitro susceptibility of yeasts (NCCLS- National Committee for Clinical Laboratory Standards- the M27A protocol)[12] and filamentous fungi[13] to current antifungal agents by Broth Dilution method has been developed. Other methods include the use of fluorescent dyes like 5, (6)-carboxyflourescein diacetate (CFDA) and bis-(1, 3-dibutylbarbituric acid) trimethine oxonol (DiBAC) to stain dead and live mycotic cells for in vitro testing.[14] Diagnostic strategies to detect circulating antigens and polymerase chain reaction based detection systems have been explored to improve identification prior to the progressive advanced disease.[15] The definitive diagnosis of invasive aspergillosis is based on showing the hyphal invasion in tissue specimens together with a positive culture for Aspergillus species from the same specimen. For early diagnosis of aspergillosis, detection of circulating fungal antigens and DNA seems to be a promising, rapid and sensitive diagnostic tool.[16] Caspofungin acetate (MK-991, formerly L-743, 872) Mechanism of action Unlike currently available agents (polyenes, pyrimidines, azoles) that exert their effect on the fungal cell membrane, echinocandins block the synthesis of b (1,3)-d-glucan, a homopolysaccharide component of the cell wall in many pathogenic fungi.[21] The rope-like glucan fibrils and chitin impart strength and shape to the cell wall and play an important role in cell division and cell growth.[22],[23] This process has no counterpart in mammalian eukryotic cells. CAS causes in vitro concentration-dependent cell death i.e., fungicidal, in yeasts and dimorphic fungi such as Candida albicans. Its effect on Aspergillus fumigatus is less well understood, possibly by killing the cells at the active centers for new cell wall synthesis within A. fumigatus hyphae when they are exposed to CAS. The minimal inhibitory concentrations (MIC) and minimal fungicidal concentrations (MFC) for echinocandins are low for a broad spectrum of fungi. Spectrum of activity CAS has a broad spectrum of antifungal activity both in vitro and in vivo. It is active against Aspergillus spp. like A. fumigatus, A. flavus, A. niger, A. terreus, and A. nidulans and Candida spp. (the most common cause of nosocomial fungal infections) like C. albicans, C. glabrata, C. krusei and C. tropicalis, including non-albicans species and isolates resistant to other drugs. In animals, it also has activity against the cyst form of Pneumocystis carinii.[24] The drug has little or no activity against Cryptococcus neoformans[25] or Mucor spp. In an animal model of coccidioidal meningitis (Coccidioides immitis), it was found that CAS might have a role in the treatment of progressive nonmeningeal coccidioidomycosis.[20] Pharmacokinetics In humans, CAS is not absorbed from the gastrointestinal tract, therefore it is not available for oral administration. The proposed susceptibility breakpoint for CAS against Candida spp. is a MIC of £1 mg/mL. Plasma concentration at 1 and 24 hours is 10.45 mg/L and 1.19 mg/L with an area under the plasma concentration curve of 104.79 mg/L.h. It has a volume of distribution of 9.67 L, is extensively bound to albumin (97%), has a plasma elimination half-life of 9 to 11 hours and is metabolized by peptide hydrolysis and N-acetylation to inactive metabolites in the liver.[26] It is not metabolized by the CYP450 enzyme system.[19] Hepatic metabolism is the primary route of excretion with kidneys eliminating less than 2% of the unchanged drug. Hepatotoxicity is not observed at therapeutic concentrations used in humans but was seen at substantially higher doses. In elderly volunteers (>65 years), there was a moderate increase in plasma concentrations after a single dose of 70 mg when compared with healthy (<45 years) volunteers, thereby suggesting that there might not be any need to adjust dosage in elderly patients. Its dosage need not be adjusted in renal insufficiency and mild hepatic disease, though use of CAS in severe hepatic disease has not been studied.[26] The exposure of the small intestine, lung and spleen to CAS was similar to that of plasma, while exposure of the heart, thigh and brain was lower than that of plasma.[27] When combined with other antifungal agents, CAS produces a synergistic or additive effect against a variety of clinically important fungi, though it needs further evaluation.[28] Efficacy CAS is as effective as AMB for the treatment of invasive candidiasis and more specifically, candidemia. In a double-blind trial in 224 patients, the efficacy of CAS was similar to that of AMB with successful outcomes in 73.4% of the patients treated with CAS and in 61.7% of those treated with AMB. CAS was superior, with a favorable response in 80.7% of patients, as compared with 64.9% of those who received AMB. CAS was as effective as AMB in patients who had candidemia (favorable response in 71.7% and 62.8% of patients, respectively).[29] Adverse effects The most commonly reported adverse effects with CAS are histamine-type reactions like fever and rash, infusion-related reactions including phlebitis, transient elevations in liver transaminase levels,[30] headache, nausea and anemia. Facial flushing has occurred during infusion. In animals, it has been found to be embryotoxic. Pulmonary infiltrates and hypercalcemia are two serious drug-related adverse events reported.[26] In a study of 623 patients, no serious clinical or laboratory drug-related adverse event was noted.[30] Comparatively, CAS has been related with significantly fewer drug-related adverse events than AMB, hence better tolerated.[24], [31]Comparative studies with other antifungals [Table - 2] In vitro studies: In a study, the activities of FLUC, ITRA, AMB and CAS were compared against 178 blood stream Candida spp. isolates from cancer patients. CAS was found to be the most active agent (MIC90 0.19-0.5 mg/l) against C. albicans, C. glabrata and C. tropicalis. It also showed substantial activity against azole-susceptible and azole-resistant Candida.[32] In another study, the activities of FLUC, AMB and CAS against biofilms were compared by the time-kill method. CAS displayed the most effective pharmacokinetic profile with ³ 99% killing, while FLUC was ineffective against C. albicans biofilms, and killing of biofilm cells was suboptimal at therapeutic concentrations of AMB.[33] The activities of CAS and ANIDU were evaluated alone and in combination with FLUC using time-kill methods against isolates of Candida albicans, C. glabrata, C. tropicalis, C. krusei and Cryptococcus neoformans in one study. Combinations of FLUC and CAS or ANIDU showed indifferent results but also did not produce any antagonistic activity.[34] In one study CAS and ANIDU were compared with ITRA, FLUC, AMB and FC against 400 bloodstream isolates of Candida spp. obtained from >30 different medical centers. Both CAS and ANIDU were very active against all Candida spp. isolates (MIC90, 0.25 and 1 mg/mL, respectively). CAS was 2 to 256-fold more active than ITRA, FLUC, AMB (except against C. parapsilosis) and FC (except against C. glabrata and C. parapsilosis). ANIDU was comparable to CAS, but was 4-fold less active against C. tropicalis and C. parapsilosis. All the isolates for which FLUC and ITRA had elevated MICs (³ 64 and ³1 mgm/mL, respectively) were inhibited by £ 0.5 mg/mL of CAS and ANIDU. These results suggest that both CAS and ANIDU possess promising antifungal activity.[35] In a study the in vitro activity of ANIDU, CAS, ITRA, AMB and FC was investigated against 51 clinical isolates of filamentous fungi, including A. flavus (10), A. fumigatus (12), Fusarium spp. (13), Rhizopus spp. (6), Pseudallescheria boydii (5) and one isolate each of Acremonium spp., A. niger, A. terreus, Paecilomyces spp. and Trichoderma spp. ANIDU was 2 to 4-fold more active than CAS against A. flavus, A. fumigatus and Trichoderma spp. Both ANIDU and CAS were considerably more active (MIC90 of 0.03-0.12 mg/mL) than ITRA, AMB and FC against Aspergillus spp., but were less active than ITRA and AMB against Rhizopus spp. CAS was more active than ANIDU or ITRA against Acremonium spp., Paecilomyces spp. and P. boydii. Therefore, ANIDU and CAS showed promising activity against Aspergillus spp. and other species of filamentous fungi.[36] In vivo studies: In a double-blind trial involving 224 patients, CAS and AMB deoxycholate were compared for the primary treatment of invasive candidiasis.[29] A modified intention-to-treat analysis showed that the efficacy of CAS and AMB was similar with successful outcomes in 73.4% and 61.7% respectively. CAS was as effective as AMB in patients who had candidemia with a favorable response in 71.7% and 62.8% of patients, respectively. There were significantly fewer drug-related adverse events with CAS than with AMB. No antagonism between them was seen against A. fumigatus, A. flavus, A. niger and A. terreus in vitro, although some synergistic additive activity was observed.[29] A double-blind randomized, multicentric trial was conducted to assess the efficacy, safety and tolerability of CAS and AMB in adults with symptomatic Candida esophagitis. By using modified intenton-to-treat analysis, endoscopically verified clinical success was achieved in 74% and 89% of patients receiving CAS 50 and 70 mg/day, respectively and in 63% of patients receiving AMB 0.5 mg/kg/day. Therapy was stopped due to drug-related adverse events in 24% of patients on AMB and in 4% and 7%, of patients who received CAS 50 and 70 mg/day respectively. CAS appears to have similar efficacy and better tolerability than AMB for the treatment of esophageal candidiasis.[37] In a double-blind randomized trial, the efficacy and safety of CAS (50 mg) was compared with FLUC (200 mg, i.v.) in adult patients with candida esophagitis. Eighty-seven per cent patients in this modified intention-to-treat analysis had HIV infection (median CD4 count of 30 cells/mm). C. albicans was the predominant isolate in this study. Favorable response rates were seen in 81% patients with CAS and in 85% patients with FLUC. By the fifth day of treatment, symptoms resolved in >50% patients with both agents. Therapy was discontinued in 1 patient (receiving FLUC) due to a drug-related adverse event. Symptoms recurred 4 weeks after stopping the drugs in 28% patients given CAS and in 17% patients given FLUC (P = 0.19).[38] Pre-clinical and clinical studies show that combinations of echinocandin with azoles and AMB do not produce antagonistic effects, rather may produce synergistic effects against pathogenic fungi.[39],[40],[41] The usefulness of such combinations is emerging in invasive aspergillosis management.[42] Therefore, combinations of these agents may warrant future clinical evaluation. Drug interactions CAS is not metabolized by the CYP450 enzyme and due to its different clearance mechanism it interacts minimally with other drugs. Co-administration with cyclosporine increased its plasma levels by 35% and caused transient liver transaminase abnormalities. Concurrent treatment with efavirenz, nelfinavir, phenytoin, dexamethasone, rifampicin and carbamazepine may require increasing dosage of CAS. It decreases serum levels of tacrolimus by about 20-25% when the two are co-administered. It does not interact with AMB or mycophenolate mofetil. No interactions have been reported with oral ITRA (200 mg/day for 14 days).[26] Resistance A genetic study in the yeast model of Saccharomyces cerevisiae has shown that mutations in FKS1 and FKS2 genes result in CAS resistance. The SBE2 cDNA plasmid conferred galactose-dependent CAS resistance when transformed back into the wild-type S. cerevisiae. The SBE2 deletion mutant was hypersensitive to CAS. Therefore, over expression of SBE2p under the regulated control of GAL1 promoter may result in CAS resistance in S. cerevisiae. This transport pathway may provide insight into the tolerance/ lack of sensitivity to CAS by some pathogenic fungi.[43] Fungal melanins might protect C. neoformans and H. capsulatum from the effects of AMB and CAS.[44] Dosage The recommended dosage of CAS in adults is 70 mg, i.v. on Day 1 followed by 50 mg/d given as a single dose over one hour with the duration of treatment depending on the severity of the patient′s underlying condition and the clinical response. Dose adjustment based on age, sex, race or renal function does not appear to be necessary, although patients with moderate hepatic insufficiency should receive a lower maintenance dose. Moreover, it is an expensive agent costing $ 9,875 (about Rupees 4.5 lakhs) for an average treatment cycle (34 days) in a dosage of 50 mg daily.[17] Micafungin (FK-463; [MICA] It is a new lipopeptide echinocandin with a broad-spectrum in vitro and in vivo antifungal activity, against both Aspergillus and Candida species. The mechanism of action is similar to CAS. MICA exhibits potent activity against Aspergillus species. It is also active against the dematiaceous fungi Cladosporium trichoides, Exophiala spinifera, Fonsecaea pedrosoi, and Exophiala dermatitidis except for certain clinical isolates. However, it had no activity against Fusarium solani, Pseudallescheria boydii, and the zygomycetes Absidia corymbifera, Cunninghamella elegans, Rhizopus oryzae and Rhizopus microsporus var. rhizopodiformis. Hence, MICA has potential utility for the treatment of infections caused by the Candida and Aspergillus species and dematiaceous fungi.[45] Pharmacokinetics After administration of a single (0.5 and 2 mg/kg, i.v.) dose of MICA to rabbits, the mean peak plasma drug concentrations were 7.62 and 16.8 mg/ml respectively, the area under the concentration-time curve from 0 to 24 hours ranged from 5.66 to 21.79 mg x h/ml, the apparent volume of distribution at steady state ranged from 0.296 to 0.343 L/kg and the elimination half-life ranged from 2.97 to 3.20 h, respectively. No significant changes in the pharmacokinetic parameters and no accumulation were noted after multiple dosing. Thirty minutes after the last of eight daily doses, mean tissue MICA concentrations were highest in the lungs (2.26 to 11.76 mg/g), liver (2.05 to 8.82 mg/g), spleen (1.87 to 9.05 mg/g) and kidney (1.40 to 6.12 mg/g). While MICA was not detectable in the cerebrospinal fluid, the concentration in brain tissue ranged from 0.08 to 0.18 mg/g. Therapeutic drug concentrations in plasma and tissues can be achieved at 0.5 to 2 mg/kg dosage of MICA at common sites of invasive fungal infections.[46] Safety and efficacy In one study, MICA was well tolerated by the mice and was much more effective than AMB or FLUC against an AMB and FLUC-resistant C. tropicalis specimen at a dose of 2-10 mg/kg body weight.[47] MICA appears to be a promising agent for invasive fungal infections but requires further clinical evaluation. It is in phase III clinical trials. Anidulafungin (LY303366; [ANIDU] It is a new echinocandin with promising broad-spectrum, antifungal activity in vitro and in vivo with a mechanism of action similar to CAS. Spectrum of activity Efficacy In one study, there was no relationship between FLUC and ANIDU MICs for C. albicans or non-albicans species. For all isolates, geometric mean (GM) MIC values (in mg/L) were: ANIDU -0.011, FLUC -8.72, FC -0.393, AMB -0.046. C. parapsilosis and C. guilliermondii were found to be significantly less susceptible to ANIDU than all other species (P ³ 0.05). For all isolates, GM MFC values (in mg/L) were: ANIDU 0.032 and AMB 0.143.[49] The in vitro activities of ANIDU, ITRA and AMB were assessed against 60 Aspergillus isolates, including isolates of A. fumigatus (35), A. terreus (8), A. flavus (8), A. niger (8) and A. nidulans (1). MFCs were 0.018, 19.76 and 12.64 mg/L for ANIDU, ITRA and AMB, respectively. ANIDU was fungicidal in 86.7% isolates (98% killing). In comparison, ITRA and AMB were fungicidal for 35% and 70% of isolates respectively (99.99% killing).[50] In a temporarily neutropenic murine model of invasive aspergillosis against AMB-susceptible (AMB-S) and AMB-resistant (AMB-R) A. fumigatus isolate based on in vivo response, 4 doses (1, 2.5, 10, and 25 mg/kg of body weight) of ANIDU were compared with AMB (0.5 to 5 mg/kg). AMB at 0.5 mg/kg and ANIDU at 1 mg/kg yielded 10 to 20% survival rates for mice infected with either AMB-S or AMB-R isolates. AMB at other dosages yielded a 70 to 100% survival rate for mice infected with AMB-S and 10 to 30% survival rate for mice infected with AMB-R (P = 0.01 to 0.04 compared with AMB-S). Against both isolates, ANIDU at 2.5, 10 and 25 mg/kg produced a survival rate of 70 to 80%, which was as effective as AMB for AMB-S, but superior to AMB for AMB-R (P < 0.03 to 0.0006). For AMB-R, ANIDU at 10 and 25 mg/kg/day was superior to AMB at 2 and 5 mg/kg/day in reducing tissue colony counts (P = 0.01 to 0.003) and for AMB-S, AMB at 5 mg/kg/day and at 5 mg/kg in 4 doses was more effective than all 4 regimens of ANIDU in reducing renal culture counts (P = 0.01 to 0.0001). ANIDU appears to be effective against AMB-susceptible and -resistant A. fumigatus infection in this model.[51] Therefore, ANIDU might have efficacy similar to CAS, FLUC, FC, ITRA and AMB.[35],[36] Combinations of FLUC and CAS or ANIDU showed indifferent results but also did not produce any antagonistic activity.[34] Thus, by virtue of its novel mechanism of action, it can be tried in combination with other antifungal agents for severe fungal infections. ANIDU is in phase III clinical trials and needs more clinical evaluation on efficacy, safety and tolerability factors. Current status CAS among echinocandins has been studied vastly and offers apparent exciting advantages of a broad spectrum of activity including strains of fungi resistant to other antifungal agents, tolerability profile, with almost no nephrotoxicity and hepatotoxicity. Although additional studies are needed, CAS appears to be a promising agent for the treatment of patients with difficult-to-treat or life-threatening fungal infections and is FDA approved. Clinical trials are required to ascertain the safety of echinocandins in special groups-pediatric, pregnant and nursing mothers. ANIDU and MICA are in phase III clinical trials. Echinocandins thus provide an exciting option for combination therapy with other antifungal agents in fulminant fungal infections.REFERENCES
Copyright 2004 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph04027t2.jpg] [ph04027t1.jpg] [ph04027f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}