 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
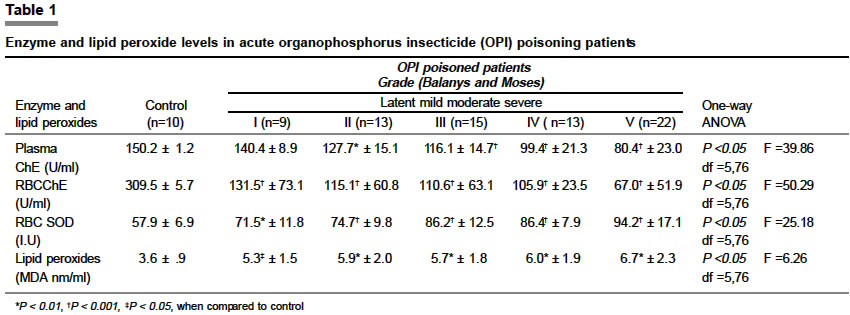
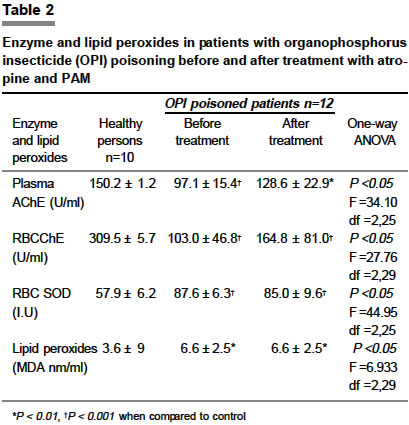
Indian Journal of Pharmacology, Vol. 36, No. 2, April, 2004, pp. 76-79 Research Paper Oxidative stress and antioxidant status in acute organophosphorous insecticide poisoning Vidyasagar J, Karunakar N, Reddy MS, Rajnarayana K, Surender T, Krishna DR Department of General Medicine, Mahatma Gandhi Memorial Hospital, Warangal Code Number: ph04029 ABSTRACT Objective: To study the antioxidant status and the extent of oxidative stress in patients with organophosphorus insecticide (OPI) poisoning before and after specific treatment. Material and Methods: The study was conducted in eighty-four OPI poisoned patients. Superoxide dismutase (SOD) and malonyl aldehyde (MDA) levels were estimated as an index of antioxidant status and oxidative stress respectively and comparisons were made (a) between different grades of poisoning based on clinical features and anticholinesterase (AChE) levels, (b) before and after therapy with atropine sulfate plus pralidoxime (PAM) and (c) between healthy control subjects and OPI poisoned patients. Results: There was a progressive fall in both the RBC and plasma AChE levels which correlated with the severity of poisoning. Upon therapy, profound improvement in the AChE levels was observed (an increase by 20.5% and 20.9% in RBC and plasma AChE levels respectively). There was also an increase in the MDA levels which nearly doubled in OPI poisoned patients who failed to survive (3.6 + 0.92 to 6.7 + 2.3 nM/ml). SOD levels increased parallel to the severity of poisoning, but did not normalize after therapy. Conclusion: The increased level of MDA in OPI poisoned patients who failed to survive was probably reflective of accelerated lipid peroxidation, cell damage and death (oxidative stress). Significant improvement was noticed in the AChE (serum and RBC) levels of patients with specific treatment but without much change in the antioxidant status as reflected by the SOD and MDA levels.INTRODUCTION Organophosphates and carbamates are the insecticides most commonly used worldwide in the pest control of crops. With green revolution and industrialization, they have become household items of the agriculturists. Unfortunately, because of their easy availability and accessibility, they have also been commonly abused for suicidal purpose in the developing countries. According to WHO, three million cases of acute poisoning occur annually, of which about 2,20,000 die. Of these, 99% of the fatal poisonings occur in developing countries, particularly among farm workers.[1] Despite an increased incidence of organophosphorus insecticide (OPI) poisoning, the exact micromolecular changes that take place remain elusive. Till date, atropine and oximes continue to occupy the prime position in the specific management of OPI poisoning.[2] Clinical manifestations of OPI poisoning are caused by excessive synaptic accumulation of acetylcholine (ACh).[3] Organophosphorus compounds irreversibly inhibit the enzyme acetylcholinesterase (AChE), resulting in excessive accumulation of ACh, leading to the paralysis of cholinergic transmission in the CNS, autonomic ganglia, parasympathetic nerve endings, some sympathetic nerve endings and neuromuscular junction.[4] It is reported that OPIs, besides their inhibitory effect on AChE, also induce changes characteristic of oxidative stress.[5] Superoxide dismutase (SOD), whose substrate is a free radical (superoxide anion; O2·-) catalyzes dismutation reaction resulting in the generation of hydrogen peroxide (H2O2). This H2O2 is decomposed to water and molecular oxygen by the action of catalase. When the free radical production overwhelms the endogenous antioxidant levels, they cause considerable cell damage/death. All the major biomolecules like lipids, proteins, and nucleic acids may be attacked by free radicals, but lipids are probably the most susceptible.[6] The oxidative destruction of lipids (lipid peroxidation) is a destructive, self-perpetuating chain reaction, releasing malonyl aldehyde (MDA) as the end product.[7] In view of the possible oxidative stress involved in OPI poisoning, it has been decided to estimate the levels of SOD and MDA as an index of antioxidant status and oxidative stress respectively, and to see whether any difference existed in these parameters before and after therapy with atropine sulfate plus pralidoxime (PAM). MATERIAL AND METHODS Subjects The severity of poisoning was graded according to the method of Balany and Moses (1968). Grade 1: no signs and symptoms, Grade 2: symptoms like vomiting, diarrhea, abdominal pain and giddiness, Grade 3: pupillary constriction with or without the symptoms mentioned above, Grade 4: pulmonary edema with or without the findings of Grades 2 and 3, and Grade 5: unconsciousness with components of Grades 2 to 4. The commonest complication encountered was respiratory failure necessitating assisted ventilation. Collection of samples Cholinesterase estimation Bromothymol blue, 0.5 ml solution was diluted with 3.8 ml of distilled water, and 0.2 ml of 15% acetylcholine chloride was added. To it 100 µl of the plasma /RBC lysate was added and the change in the color was read at 620 nm at 37°C, after 30 minutes. A standard graph was plotted using acetic acid 0.015N in concentrations of 10, 20, 50, 100 and 200 micromoles. RBCs were extracted by first adding distilled water (3 ml) followed by precipitation of the hemoglobin with acetone (2 ml), and centrifugation at 3000 rpm. The supernatant was used for estimation of RBC AChE. The unit of AChE activity was defined as the micromoles of acetic acid liberated from 1 ml of plasma or RBC lysate in 30 min at 37°C. Superoxide dismutase (SOD) estimation Two ml of packed cells were lysed by addition of an equal volume of cold deionized water. Hemoglobin was then precipitated by adding chloroform: ethanol (1.5: 1) mixture. The mixture was centrifuged at 3000 rpm for 15 min, and the SOD activity was measured in the supernatant. To 0.88 ml of riboflavin (Acto Pharma, Warangal, AP, India) solution (1.3 X 10-5 mM in 0.01M potassium phosphate buffer, pH 7.5) 60 µl of O-dianisidine (Sigma St. Louis, USA) solution (10-2 mM in ethanol) was added. To this 1 ml of distilled water was added and kept away from light. Hundred µl of the separated SOD was added and optical density (OD) measured at 460 nm using the spectrophotometer. The cuvette was then transferred to the illumination box (40 Watt white fluorescent tube) for exactly 4 min and the OD was remeasured against blank containing ethanol in place of enzyme. The SOD was estimated from the standard graph plotted using different concentrations of pure bovine SOD. Lipid peroxides estimation To 0.5 ml of the serum, 0.5 ml of 30% trichloroacetic acid (TCA) (BDH Fine Chemicals, Mumbai) and 100 µl of 1% TBA reagent were added. The tubes were covered with aluminum foil and kept in a shaking water bath for 60 min at 80°C. The tubes were then kept in ice-cold water for 10 min followed by centrifugation at 3000 rpm for 15 min. The absorbance of the supernatant was read at 540 nm at room temperature against blank. The concentration of MDA was read from standard calibration curve plotted using 1, 1, 3, 3′ tetra-ethoxy propane (BDH Fine Chemicals, Mumbai). The results were presented in nanomoles of MDA per ml of serum. The data were analyzed using one-way ANOVA, followed by Student-Neuman-Keul′s multiple comparison test. P values < 0.05 were considered significant. RESULTS AChE SOD and MDA The mean + SD serum level of MDA in healthy subjects in the present study was 3.6 + 0.9 nM/ml and it nearly doubled in OPI poisoned patients (Grade 5, 6.7 + 2.3 nM/ml). With an increase in the severity of poisoning there was a corresponding increase in the MDA levels [Table - 1] . DISCUSSION OPI poisoning is primarily a problem of developing countries like India. In the present study, inhaled OPI poisoning constituted about 10% of the cases and the remaining 90% were suicidal attempts by the oral route. This is in contrast to figures reported from the developed countries like Japan where accidental exposure formed the bulk.[11] The role of oxygen free radicals (OFR) has been well established in many chronic disorders. The significance of the implication of OFR in an acute condition like OPI poisoning has not been investigated so far. The effects of organophosphates on fish revealed that besides AChE inhibition, there were changes characteristic of oxidative stress.[5] In humans, OPIs were shown to reduce the total cholesterol and phospholipid level of RBC membrane following phosphamidon and malathion, and increase lipid peroxides level following malathion.[12] The basis of OPI toxicity in the production of OFR may be due to a) their "redox-cycling" activity - they readily accept an electron
to form free radicals and then transfer them to oxygen to generate superoxide
anions and hence hydrogen peroxide through dismutation reaction.[13] The efforts of the endogenous antioxidant enzymes to remove the continuously generated free radicals initially increase due to an induction but later enzyme depletion results, resulting in oxidative cell damage.[14] Hence, when the generation of reactive free radicals overwhelms the antioxidant defense, lipid peroxidation of the cell membrane occurs. This causes disturbances in cell integrity leading to cell damage/death. In the present study the increase in AChE levels indicated the severity of poisoning while SOD and lipid peroxide levels served as an index of the antioxidant status and oxidative stress respectively. The clinical manifestations and pathophysiology of OPI poisoning in relation to AChE levels has been well established. Organophosphates inhibit AChE, but are more selective for RBC AChE, than plasma pseudo ChE. A progressive decrease in AChE levels with an increasing severity of poisoning, reflect a proportionate amount of pesticide consumed and absorbed. It has been well established that therapy with PAM (AChE reactivator) reverses the inhibited levels of AChE.[4] SOD, which catalyzes the dismutation of superoxide anion radicals to O2 and H2O2, has been implicated as an essential defense against the potential toxicity of oxygen. It is considered to serve as a cellular defense against the potentially harmful effects of superoxide anion generated by a wide variety of biological reactions. In the present study, the increased SOD levels indicate an elevated antioxidant status. A parallel increase in SOD levels with an increase in the severity of poisoning shows that, more the stress, more the free radicals are generated. This is additionally corroborated by the increased lipid peroxide levels (MDA). The free radical production is so high that it even overwhelms the elevated antioxidant (SOD), failing to check lipid peroxidation. The involvement of free radicals other than superoxide anions like hydroxyl free radical could not be ruled out, since the increased SOD levels were only partially effective in combating the oxidative damage. This calls for the investigation of the involvement of other antioxidant enzymes (catalases, glutathione peroxidases) in conditions like OPI poisoning. In patients who failed to survive, a sharp increase in the lipid peroxide levels could have accelerated lipid peroxidation of the cell membrane leading to massive cell damage/death. Current therapy has not shown any defense against this process. It is concluded that that there was a considerable increase in lipid peroxide levels indicating an enormous oxidative stress in OPI poisoned patients. Significant improvement was noticed in the AChE levels (serum and RBC) with treatment but without much change in the antioxidant status. ACKNOWLEDGEMENTS The authors are thankful to the University Grants Commission and the Council of Scientific and Industrial Relations for their financial assistance. REFERENCES
Copyright 2004 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph04029t1.jpg] [ph04029t2.jpg] |
| |||||||||

{kind=link}
{kind=link}