 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
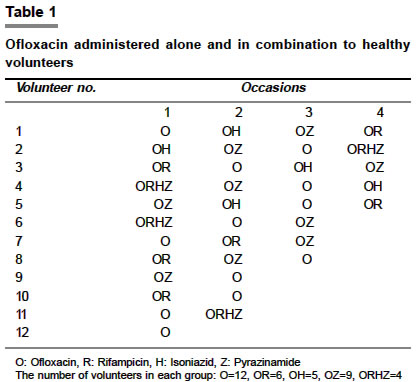
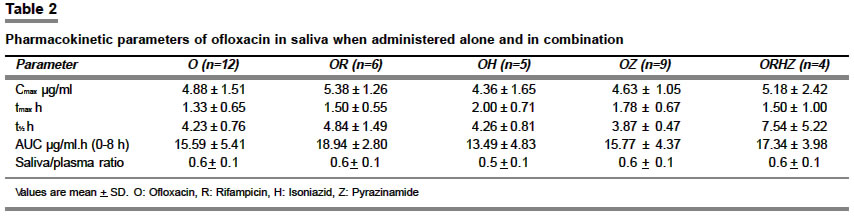
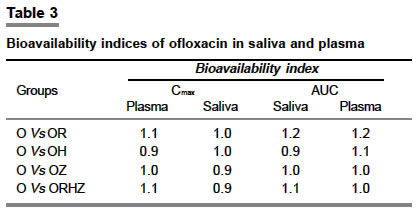
Indian Journal of Pharmacology, Vol. 36, No. 2, April, 2004, pp. 80-83 Research Paper Ofloxacin pharmacokinetics in saliva Hemanth Kumar AK, Gurumurthy P Department of Biochemistry, Tuberculosis Research Centre (ICMR), Chennai - 600031 Code Number: ph04030 ABSTRACT Objective: To study the pharmacokinetics of ofloxacin using salivary drug concentration when administered alone or in combination with rifampicin (R), isoniazid (H) and pyrazinamide (Z) and also to assess the saliva to plasma concentration ratio. Material and Methods: Twelve healthy male volunteers were investigated on four different occasions with an interval of at least one week between occasions. They were administered ofloxacin, either alone or in combination with R, H and Z. A partially balanced incomplete block design was adopted and the subjects were randomly allocated to each group. Salivary and plasma concentrations of ofloxacin were measured at 1, 2, 3, 6 and 8 h after drug(s) administration using validated methods. Results: There were no significant differences between various pharmacokinetic parameters when ofloxacin was administered alone or in combination with R, H and Z. The mean saliva to plasma ratio of ofloxacin concentration was around 0.6. The bioavailability indices of ofloxacin in the saliva and plasma were similar in all the groups. Conclusion: Several pharmacokinetic parameters could be calculated using salivary concentrations of ofloxacin. The determination of ofloxacin levels in saliva may be useful in therapeutic drug monitoring and pharmacokinetic studies.INTRODUCTION Ofloxacin is a fluorinated carboxy quinolone exhibiting a marked bactericidal effect by inhibiting DNA gyrase.[1],[2] In vitro studies on bactericidal activity against Mycobacterium tuberculosis have suggested that ofloxacin is likely to be the most useful drug in the early stages of treatment and in preventing the emergence of resistance to other drugs.[3] Its favorable pharmacokinetic features include good oral absorption and lack of metabolism resulting in less drug interactions.[4] The determination of drug concentrations in the saliva has gained widespread acceptance in a variety of settings.[5] The estimation of drugs in the saliva has been employed for therapeutic drug monitoring and for calculation of pharmacokinetic variables.[6] The rational use of such determinations can provide knowledge of patient-specific pharmacokinetic parameters leading to improved therapy.[7] Saliva can serve as an alternative body fluid for pharmacokinetic investigations. It can be collected with minimal patient discomfort and can be easily obtained on multiple occasions. It is particularly suitable for investigations in geriatrics and pediatrics. Pharmacokinetic studies have shown that ofloxacin penetrates into saliva and its concentration correlates well with serum levels.[8] However, the data available in the published studies are inconsistent and results reported for the ratio of saliva to serum concentrations show wide variations. The present study was undertaken to evaluate the pharmacokinetics of ofloxacin in saliva when administered alone or in combination with other antituberculosis (TB) drugs, viz. rifampicin (R), isoniazid (H) and pyrazinamide (Z) and to study the ratio of the saliva to plasma concentration by measuring ofloxacin concentrations in simultaneous saliva and plasma samples in healthy volunteers. MATERIAL AND METHODS Study participantsTwelve healthy male volunteers with a mean age of 23 years (range 19-27 years) and a mean body weight of 56 kg (range 45-69 kg) participated in the study. The volunteers were assessed to be healthy on the basis of medical history, hepatic and renal function tests. None of the subjects was taking any medication one week before or during the study for any ailment and were non-alcoholics. The study protocol was approved by the Institutional Ethics Committee and written informed consent was obtained from all the volunteers. Assay for the stated contents of the drugs Study design Sample collection Assay of ofloxacin Pharmacokinetic analysis Data analysis was performed using SPSS (version 10.5) package. Differences among the treatment groups were determined using one-way ANOVA. P values <0.05 were considered significant. RESULTS Based on the salivary concentrations of ofloxacin at different time points, several pharmacokinetic variables were calculated [Table - 2]. The mean Cmax values of ofloxacin when administered alone and in combination with R, H, Z and RHZ were 4.88, 5.38, 4.36, 4.63 and 5.18 mg/ml respectively. There were no significant differences in the Cmax and the tmax of ofloxacin between the different groups. The concentrations of ofloxacin in saliva were much lower than those in plasma. The Cmax values of ofloxacin in plasma when administered alone and in combination with R, H, Z and RHZ were 7.14, 6.98, 7.19, 6.06 and 6.38 mg/ml respectively. The mean saliva to plasma ratio of ofloxacin concentrations was calculated at all time points and it was around 0.6. The correlation coefficient between plasma and saliva concentration of ofloxacin was 0.94. The mean saliva to plasma (S/P) ratio of ofloxacin concentration when given alone and in combination was compared [Table - 2]. There was no significant difference between the groups. The bioavailability indices of ofloxacin in saliva and plasma calculated on the basis of Cmax and AUC (in comparison with various combinations) are shown in [Table - 3]. They are similar in all the groups. DISCUSSION Ofloxacin has proved to be a particularly valuable addition to the available anti-TB drugs with a MIC of 1.0 mg/ml against Mycobacterium tuberculosis. The effectiveness of ofloxacin against Mycobacterium tuberculosis was studied by Crowle et al[10] and their results reveal its clinical usefulness. Using saliva instead of blood for pharmacokinetic investigations has obvious practical advantages. It is a painless, non-invasive procedure, hence suitable for the collection of multiple specimens. Variable results have been reported for the ratio of saliva to serum concentrations. Koizumi et al[11] reported a ratio of 1.0 between 2-8 h after administration of a 300 mg dose. Fujita et al[12] in their studies on patients with renal impairment had reported a ratio of 1:1 for saliva to serum concentrations. However, Warlich et al,[13] have reported a ratio of 0.6 and a close relation of levels in the saliva and serum (r= 0.99), which is consistent with our findings. The mean S/P ratio of ofloxacin was around 0.6 and this remained the same when ofloxacin was given in any combination. The S/P ratio is a possible measure of the amount of protein binding to the drug. There was a good correlation (0.94) with respect to drug concentrations. The present study shows that several pharmacokinetic parameters can be calculated using salivary concentrations of ofloxacin as can be done with plasma. The estimation of ofloxacin levels in saliva seems to be useful in therapeutic drug monitoring and pharmacokinetic studies. Based on the salivary levels, the present study compares the pharmacokinetic parameters of ofloxacin when given alone and in combination with other anti-TB drugs namely R, H and Z. The pharmacokinetic parameters such as Cmax, tmax, AUC, and t½ did not change when given in combination with other anti-TB drugs suggesting that the pharmacokinetics of ofloxacin do not get affected or altered when administered with the other anti-TB drugs. When ofloxacin was administered in combination with three other drugs, namely R, H and Z, there were variations in the pharmacokinetic parameters calculated based on the salivary estimates. This could be due to the small sample size in this group (n=4) and interindividual differences in the absorption and metabolism of the drug. The microbiological assay (MBA) employed for the estimation of ofloxacin in the saliva and plasma is very simple, specific, sensitive and reproducible, and does not require sophisticated equipment. This method was evaluated in samples wherein drug levels were also measured by HPLC according to the method of Immanuel et al.[14] A very good correlation (0.99) was observed suggesting either method may be useful for pharmacokinetic studies. It can, therefore, be concluded that for bioavailability studies, invasive blood collection can be replaced by simple non-invasive saliva collection. Further investigations are required to determine whether the concentration of ofloxacin in saliva can act as a valid index after multiple dosing. In this regard, a larger population sampling is required before any general statements regarding the utility of salivary measurements of ofloxacin can be made. ACKNOWLEDGEMENTS The authors wish to thank the volunteers for their willingness to participate in this study, Mr. L. Sekar for the statistical help and Mr. B. Doraiswamy for secretarial assistance. REFERENCES
Copyright 2004 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph04030t1.jpg] [ph04030t2.jpg] [ph04030t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}