 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
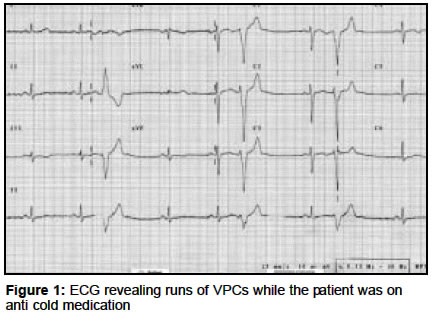
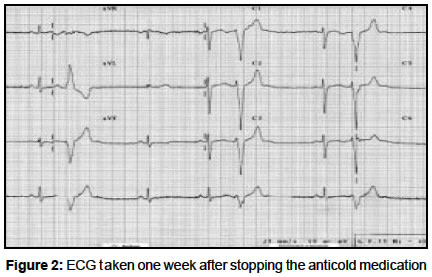
Indian Journal of Pharmacology, Vol. 36, No. 2, April, 2004, pp. 106-107 Case Report Iatrogenic uneasiness and fast forward ventricular ectopics Sivagnanam G Department of Pharmacology, Chengalpattu Medical College, Chengalpattu - 603001 Code Number: ph04041 A 23-year-old female novice, with no previous history of heart disease was prescribed On Day 2 the patient returned with complaints of uneasiness, dizziness and weakness. The patient was sent to the author for an opinion. On examination: the pulse rate - 50/min and highly irregular; temperature - normal; BP - 128/80 mm of Hg; RR - 18/min; not anemic and no pedal edema. Her menstrual history was normal with no missed periods. No member of her family has any known cardiac problem. A detailed history and clinical examination revealed no evidence of any systemic abnormality except the abnormal pulse. An immediate ECG revealed that there were runs of ventricular premature complexes (VPCs). The patient was reassured and advised to stop all medications. She was also instructed to have a cardiology consultation upon worsening of symptoms or any new adverse development. When the patient returned a week later she felt perfectly well. A repeat ECG revealed a marked reduction in the frequency of VPCs. The patient was however advised to have a specialist opinion for the VPCs. The patient could not be seen later but enquiries revealed she was doing fine. COMMENT The irregular pulse was due to VPCs, which was revealed by the ECG [Figure - 1]. In VPCs, the pulse is irregular owing to the premature beats. ′Frequently repetitive ventricular ectopic activity of a single morphology′, as seen in this case, is one form of manifestation of VPCs.[1] The presenting symptoms on Day 2 could clearly be attributed to pseudoephedrine, since several classes of drugs including sympathomimetics (epinephrine, pseudoephedrine, phenylephrine, phenylpropanolamine, amphetamine), methylxanthines (caffeine, theophylline), digitalis, cocaine and certain general anesthetics (halothane) may induce VPCs.[2] Since frequent VPCs reduce stroke volume and the cardiac output by the "halving" of the heart rate, symptoms like syncope or lightheadedness are a possibility.[3] In this case the heart rate was 56/min [Figure - 1]. Chlorpheniramine (present both in the anti-cold and anti-cough preparations), an antihistamine with anticholinergic activity also could have contributed to the exaggeration of VPCs, since decreased vagal action is also a well-known destabilizing influence on the existing electrical instability of the heart.[4] VPCs occur in many healthy individuals. In the absence of heart disease there is little or no increased risk. In patients with disturbing or disabling palpitations due to VPCs, avoidance of potentially aggravating factors (e.g. tobacco, coffee, caffeine-containing beverages, environmental stress or stimulants) should be tried before pharmacologic therapy.[2],[5] In the present case the aggravating factors were clearly the drugs (mainly pseudoephedrine and may be to a lesser extent chlorpheniramine). As mentioned earlier, all the drugs were stopped and the patient was relieved of the disturbing symptoms. There was a marked reduction in the frequency of VPCs [Figure - 2]. The patient was advised against use of cough and cold remedies on her own. She was also advised to alert the physician in future about her condition . The syndrome of right bundle branch block, S-T segment elevation in the anterior precordial leads, and risk of sudden death has been described in the literature. Such cases have no associated structural heart disease and in some, the patients are asymptomatic. It is commonest in young adult males and has been suggested as the basis for the so-called "sleep death" in young Asian males.[5] Since the patient is a young Asian female, she was advised for a specialist opinion of her condition. LESSONS
REFERENCES
Copyright 2004 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph04041f2.jpg] [ph04041f1.jpg] |
| |||||||||

{kind=link}
{kind=link}