
|
Indian Journal of Pharmacology
Medknow Publications on behalf of Indian Pharmacological Society
ISSN: 0253-7613 EISSN: 1998-3751
Vol. 36, Num. 3, 2004, pp. 133-139
|
Indian Journal of Pharmacology, Vol. 36, No. 3, June, 2004, pp. 133-139
Education Forum
Glycoprotein IIb/IIIa receptor and its inhibition: A platelet-directed therapeutic strategy
Shah HD, Goyal RK
Department of Pharmacology, L. M. College of Pharmacy, Navrangpura, Ahmedabad, Gujarat
Correspondence Address:Department of Pharmacology, L. M. College
of Pharmacy, Navrangpura, Ahmedabad, Gujarat goyalrk@rediffmail.com
Code Number: ph04049
ABSTRACT
Platelets play a key role in atherosclerosis, thrombosis and acute coronary
syndromes. Drugs that dissolve blood clot (thrombolytic agents) and that
prevent clot propagation (antiplatelet and anticoagulant agents) are used
to treat a broad array of cardiovascular diseases. Therapeutic manipulation
of platelet function has focused principally on the use of aspirin which
has proved effective in many clinical situations, despite its relatively
weak antiplatelet action as compared to newer agents like ticlopidine,
clopidogrel and more recently, platelet glycoprotein (GP) IIb/IIIa receptor
inhibitors. The platelet GP IIb/IIIa receptor has been identified as a
pivotal mediator of platelet aggregation, making it a logical target for
the control of the platelet response to vascular injury. The primary mechanism
of GP IIb/IIIa antagonists is the inhibition of the final common pathway
of platelet aggregation: fibrinogen binding to the GP IIb/IIIa complex.
Various antagonists of the GP IIb/IIIa receptor are currently receiving
considerable attention and are being investigated for various clinical
settings including angina, myocardial infarction and interventional cardiology.
It is well known that platelets play a central role in acute coronary
syndromes.[1] Understanding
the molecular mechanism that underlies the pathophysiology of acute coronary
syndromes has been critical in developing optimal pharmacological therapies.
Given the key role of thrombosis, pharmacological therapy has sought
to provide potent inhibition of both platelet aggregation and coagulation
cascade. Traditionally, antiplatelet therapy with aspirin and anticoagulation
with Unfractionated Heparin (UFH) has been the cornerstone of the management
of patients with cardiovascular diseases.[2] Aspirin,
however, blocks only one of the several signal transduction pathways
leading to platelet activation (i.e. inhibits prostaglandin G/H
synthase). Therefore, platelet activation and aggregation is effectively
allowed to continue even in its presence.[3] UFH
binds to antithrombin III, thus inhibiting the activity of the coagulation
cascade. However, UFH is ineffective against clot-bound thrombin.[4] Low
molecular weight heparin (LMWH) offered several potential advantages
over traditionally used UFH, including minimal interaction with platelets
and lower incidences of heparin-induced thrombocytopenia.[5] Additionally,
unlike UFH, LMWHs do not interact with plasma proteins, hence their anticoagulant
effects are more predictable, eliminating the need for monitoring. However,
it is a matter of concern that platelet aggregation and development of
thrombosis are relatively resistant to conventional therapy with fibrinolytics.
Newer agents like ticlopidine and clopidogrel were developed initially
as an adjunct to aspirin.[6],[7] The
antiplatelet action of ticlopidine is principally exerted by blocking
the ADP-mediated activation of platelet glycoprotein (GP) IIb/IIIa receptors.
Clopidogrel is a newer thienopyridine derivative, chemically related
to ticlopidine. It also blocks activation of GP IIb/IIIa receptors by
irreversibly inhibiting the binding of the agonists to their receptors
on the platelets, thereby affecting the ADP-dependent activation of the
GP IIb/IIIa complex.[8] Platelet
aggregation involves cross-linking of activated glycoprotein (GP) IIb/IIIa
receptors on two adjacent platelets by a single molecule of plasma fibrinogen.
The platelet GP IIb/IIIa receptor has been identified as a target for
control of the platelet response to vascular injury.[9] During
the last decade intensive efforts have been made to evaluate the role
of the GP IIb/IIIa complex in platelet-mediated thrombus formation.[10] GP
IIb/IIIa serves as the receptor on platelets that binds plasma-borne
adhesive proteins, such as fibrinogen and von Willebrand factor, thus
permitting platelet aggregation. GP IIb/IIIa receptor antagonists act
by inhibiting this final common pathway of platelet aggregation.[11] In
the present review, we have summarized the role of GP IIb/IIIa in platelet
function, its antagonists and their application as newer and safe therapeutic
agents.
Biology of platelet function
Platelet adhesion and aggregation
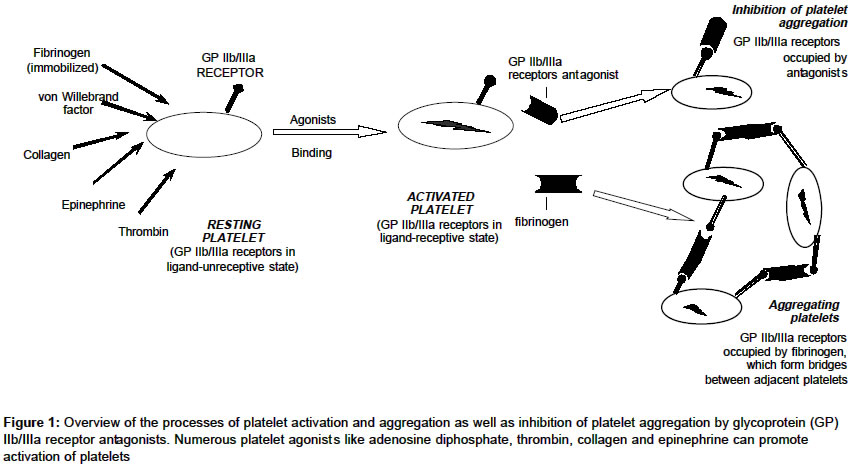
Platelet adhesion, the first step in the process of hemostasis, is triggered by damage to the vessel wall and local exposure of the sub-endothelial matrix.[9] It involves deposition of platelets from the circulation on to the newly exposed sub-endothelial surfaces and occurs almost instantaneously after vascular and tissue trauma that leads to interruption of the continuity of blood vessels.[2] Local mechanical or biochemical stimuli can induce activation of adherent platelets.[12] High shear blood flow condition can activate adherent platelets even in the absence of additional stimuli, but the process is more rapid when biochemical stimuli are involved.[2] Molecules secreted or released from platelets include platelet activators such as thromboxane A2 (TXA2), serotonin, ADP and epinephrine, and mediators of inflammation and vascular repair such as cluster determinant (CD) 40 ligand, platelet derived growth factor (PDGF)-b and tumor growth factor (TGF)-b2 Platelet activation is also characterized by changes in the platelet surface that promote coagulation and aggregation. Regardless of the mode of platelet activation, platelet aggregation is mediated by the GP IIb/IIIa receptor and it is the final common pathway in thrombus formation.[13] [Figure
- 1] depicts the role of GP IIb/IIIa in platelet aggregation. Unstimulated discoid platelets are shown with receptors for thrombin, ADP, collagen, vWF and immobilized fibrinogen. All of these are capable of stimulating platelets, inducing change in platelet shape, and activating the receptor function of GP IIb/IIIa.
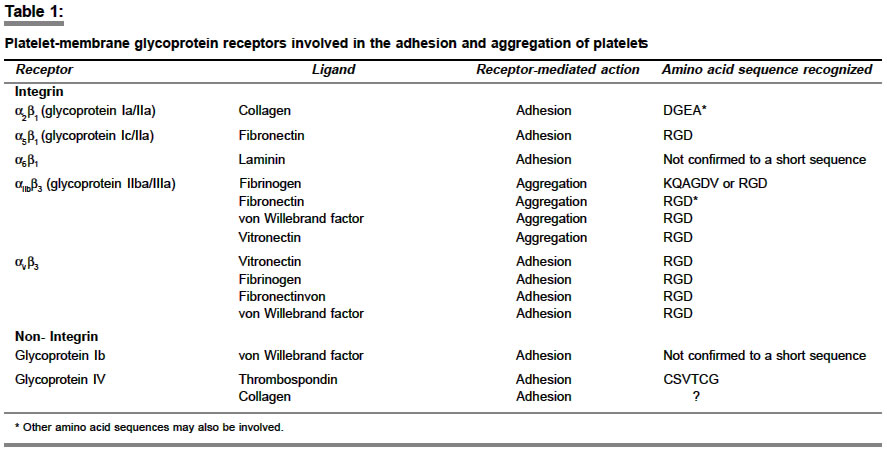
Platelet adhesion and aggregation are controlled by the activity of
the platelet membrane receptors which biochemically are GPs. According
to their genetic origin, GPs can be divided into five groups called platelet
gene families: the integrins, the leucin-rich GP family, the selectin
family, the quadraspanin family and the immunoglobulin supergene family.[12] The
thrombus formation initiated by platelet adhesion to extracellular matrix
(ECM) involves the synergistic function of at least four receptors, the
GP Ib-IX-V complex and the integrins a2b1 (GP Ia-IIa), aIIbb3 (GP IIb-IIIa)
and a5b1 (GP Ic-IIIa).[13],[15] Aggregation,
in contrast, may depend only on the GP Ib-IX-V complex and aIIbb3 [Table
- 1].[14] To
form stable bonds either with the ECM components or with other platelets,
circulating platelets must attach to a reactive substrate, resisting
the force of flowing blood, which would tend to move platelets with the
layer of fluid adjacent to the vessel wall.[14],[15] This
reactive substrate is provided by sub-endothelial and extra-vascular
ECM components during adhesion, and during aggregation activated platelets
that are already firmly adherent play this role; but in either case,
fluid drag opposes the initial establishment and subsequent enlargement
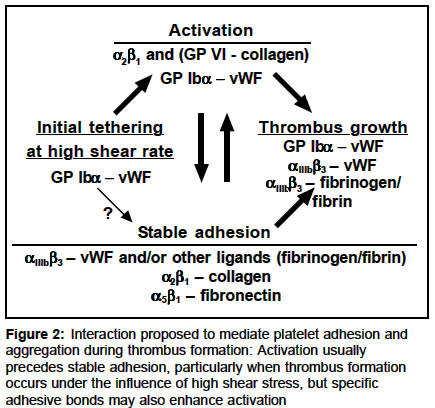
of the thrombus.[15] Interaction
proposed to mediate platelet adhesion and aggregation during thrombus
formation is depicted in [Figure - 2].
GP IIb/IIIa receptor and its role in platelet aggregation
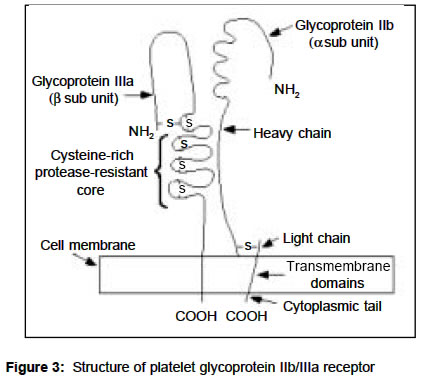
The GP IIb/IIIa receptor (aIIbb3) belongs to the integrin family of platelet receptors.[9] Its
structure has been shown in the [Figure
- 3]. The receptor consists of
two subunits, alpha and beta. The alpha subunit is of 136-kDa and consists
of a heavy chain and a light chain. The light chain has a short cytoplasmic
tail, a trasmembrane region, and a small extracellular domain; whereas
the heavy chain is entirely extracellular.[16] The beta subunit is of 92 kDa and consists of a single polypeptide of 762 aminoacids, with a short cytoplasmic tail, a single transmembrane region, and a large extracellular domain. There are various types of platelet gene families and their subtypes. Accordingly, there are different types of receptors and their sub-units (alpha and beta) differ in structure and combinations. Among various integrins, the aIIb sub-unit has been found in combination with b3 and this is found to be present in the cells of megakaryocyte lineage.[9] Both the alpha and beta subunits are non-covalently bound to each other, and calcium is required to maintain the heterodimeric structure.[17],[18] Platelet activation causes changes in the shape of platelets and conformational changes in GP IIb/IIIa receptors, transforming the receptors from a ligand-unreceptive to a ligand-receptive state[12] [Figure
- 3]. Ligand-receptive GP IIb/IIIa receptors bind fibrinogen molecules,
which form bridges between adjacent platelets and facilitate platelet
aggregation.[10],[19],[20] Inhibitors of GP IIb/IIIa receptors also bind to these receptors, blocking the binding of fibrinogen and thus preventing platelet aggregation.[21] Although the binding of fibrinogen to GP IIb/IIIa receptors is the principal mechanism for platelet aggregation,[22],[23],[24] other adhesive GPs including fibronectin, von Willebrand factor (vWF) and vitronectin also bind to these receptors.[25],[26]
Much effort has been directed towards characterizing the molecular basis for the binding of the soluble adhesive proteins vWF and fibrinogen to platelets.[27] The recognition specificity of the GP IIb/IIIa receptor is defined by two peptide sequences, through which the agonists bind to it. One is the Arg-Gly-Asp (RGD) and another sequence is Lys-Gln-Ala-Gly-Asp-Val (KQAGDV). The RGD sequence was initially identified as the adhesive sequence in fibronectin[28] but it is also present in fibrinogen, von Willebrand factor and vitronectin. All these ligands contain at least one RGD sequence, whereas fibrinogen contains two RGD sequences per half molecule.[29] The KQAGDV sequence is the other major sequence involved in the binding of fibrinogen to GP IIb/IIIa receptors and is located at the carboxyl terminus of the g-chain of fibrinogen.[30],[31] Unlike RGD, this sequence is found only in fibrinogen and is probably the predominant site for the binding of fibrinogen to GP IIb/IIIa receptors.[32],[33] Apart from fibrinogen binding, GP IIb/IIIa receptors on unstimulated platelets are also involved in binding of prothrombin, an interaction that increases the rate of prothrombin conversion to thrombin.[34]
Since the GP IIb/IIIa receptor is the final common pathway by which platelet aggregation takes place, direct inhibition of this receptor is likely to prove superior to blockers of only some of the pathways.[35] Various antagonists of GP IIb/IIIa are currently receiving considerable attention from the pharmaceutical industry and are being studied in a variety of clinical settings.[36],[37],[38],[39] Significant efforts have also been made to design potent antagonists of this final common pathway of platelet aggregation to be used as novel therapeutic strategies to inhibit thrombosis that leads to acute coronary syndromes.[40] Although several different GP IIb/IIIa antagonists have convincingly demonstrated the usefulness of this platelet-directed therapeutic strategy, a number of unsolved and sometimes misunderstood issues concerning the pharmacology and optimal clinical usefulness of these agents remain to be explored.
GP IIb/IIIa receptor antagonists
GP IIb/IIIa antagonists belong to an unusual drug class, in part because platelet stimulation, which occurs during arterial thrombosis, may change the number of functional GP IIb/IIIa complexes on the platelet surface and also because the receptor cannot be saturated, but rather is titrated to optimize antithrombotic activity and minimize antihemostatic activity.[10],[41] Potent
agonists such as thrombin can cause up to a 50% increase in the
number of GP IIb/IIIa molecules exposed on the platelet surface; therefore,
receptor occupancy after stimulation becomes an important consideration
to predict antithrombotic efficacy.[41]
The first GP IIb/IIIa antagonist developed for clinical investigation was the murine monoclonal antibody M7E3.[42] M7E3 demonstrated prevention of platelet aggregation by inhibiting fibrinogen binding.[42] Later abciximab, a Fab chimera that retains the mouse-derived variable portion of M7E3 joined the constant region of human IgG Fab. It has undergone extensive clinical evaluation and is approved by regulatory agencies worldwide as an adjunct to coronary intervention.[43],[44],[45] Natural products have also been screened extensively for activity against GP IIb/IIIa receptors. Trigramin, isolated from the venom of the viper Trimeresurus gramineus, is a potent inhibitor of ligand binding to the GP IIb/IIIa receptors.[12] Synthetic linear peptides based on the RGD template have also been investigated. These include agents like G 4120 and MK-856.[46] However, these had relatively little activity and were more resistant to enzymatic degradation. Replacement of the arginine group in the RGD sequence with an amidino or benzamidino containing group increased the resistance to enzymatic degradation. Agents in this group include lamifiban (previously known as Ro 44-9883) and tirofiban (previously known as MK-383). A novel non-peptide GP IIb/IIIa antagonist XV 459[47] and another long acting potent fibrinogen receptor antagonist L-738,167[48] are being tested for their antithrombotic efficacy. However, the four clinically used parenteral GP IIb/IIIa antagonists include abciximab, the cyclic peptide eptifibatide, the non-peptide tirofiban, and the peptidomimetric lamifiban.[49]
Oral GP IIb/IIIa antagonists are being investigated for secondary prevention of cardiovascular morbidity and mortality.[42] These include xemilofiban, orbofiban, sibrafiban (SC-54684) and roxifiban.[49] Roxifiban has been tested in the Roxifiban Oral Compound Kinetic Evaluation Trial (ROCKET-I) for its effect on platelet aggregation and major receptor expression in patients with CAD.[50]
Properties
Although all GP IIb/IIIa inhibitors have a rapid onset of action, the return of platelet function to normal following drug discontinuation varies according to the individual agent.[51],[52] The duration of the action of eptifibatide and tirofiban is short because they bind reversibly to the GP IIb/IIIa receptor and have a short half-life. Therefore, within a relatively short time after the discontinuation of these agents, there is little or no increased risk of bleeding.[53] Abciximab has a short plasma half life but a long duration of action due to its high affinity binding to the receptors. Both eptifibatide and tirofiban HCl are highly specific for the platelet receptor GP IIb/IIIa, whereas abciximab also binds to the related integrins vitronectin and Mac-1.[54],[55] Due to its relatively large size and murine origin, abciximab is capable of eliciting an antibody response, which has not been observed with either eptifibatide or tirofiban HCl.[56] The P1A2 genotype of the GP IIb/IIIa receptor appears to be associated with adverse outcome in patients treated with oral GP IIb/IIIa antagonists. Thus, P1A2 polymorphism of these receptors is now emerging as a probable determinant of the response to antiplatelet agents.[57] Soluble CD40 ligand (sCD40L) is a prothrombotic and proinflammatory protein that is released by platelet activation and subsequent aggregation by GP IIb/IIIa activity. Therefore, GP IIb/IIIa antagonists may not only inhibit thrombosis through blockade of platelet aggregation but may also inhibit inflammation and thrombosis through blockade of sCD40L release.[58] Clinical trials overview
GP IIb/IIIa receptor antagonists in interventional cardiology
Five large, randomized, placebo controlled trials of GP IIb/IIIa antagonists define our current knowledge regarding the adjunct use of these agents during coronary intervention. These include EPIC (Evaluation of M7E3 for the Prevention of Ischemic Complication) trial, EPILOG (Evaluation in PTCA to Improve Long term Outcome with abciximab GP IIb/IIIa Blockade) trial, CAPTURE (c7E3 Fab Antiplatelet Therapy in Unstable Refractory angina) trial, IMPACT-II (Integrelin [eptifibatide] to Minimize Platelet Aggregation and Coronary Thrombosis II) trial and RESTORE (Randomized Efficacy Study of Tirofiban for Outcome and Restenosis) trial. In each trial the study was initiated before coronary intervention. The EPIC trial showed conclusively that administration of abciximab in the form of a bolus followed by a low dose infusion for 12 h produced significant reduction in 30 day combined primary endpoints (death, non-fatal myocardial infarction, CABG or emergency PTCA, stent insertion for procedural failure and balloon pump insertion for refractory angina).[8],[59] The
EPILOG trial compared abciximab and standard dose heparin (100 U/kg bolus
and additional to maintain ACT>300s), with abciximab and low dose heparin (70 U/kg bolus and ACT>200s)
and with placebo and standard dose of heparin.[45] At the end of 30 days, composite endpoints like death, myocardial infarction (MI) and revascularisation were significantly reduced in low dose heparin with abciximab group as well as in standard dose heparin with abciximab group. The CAPTURE trial provided evidence that, in patients with refractory unstable angina, pretreatment with abciximab may reduce the incidence of MI prior to PTCA.[60]
The 30 day results of the RESTORE trial showed that tirofiban produced a decrease in composite endpoint of death, MI, CABG, Target vessel revascularisation (TVR) or stent insertion for threatened closure.[61] The IMPACT-II trial compared a low dose infusion regime of eptifibatide (0.5 mg/kg/min) with a high dose infusion (0.75 mg/kg/min) as well as with placebo.[62] The results suggested that the low dose infusion was better than the high dose infusion regime. However, there was no difference between the low dose infusion regime and the placebo group in the composite end points (death, MI, urgent revascularization by PTCA or CABG, or stent replacement for abrupt closure). The recently published Evaluation of Platelet Inhibitor for stenting (EPISTENT) trial compared the use of abciximab in conjunction with angioplasty or stenting without abciximab.[63] The 30 day primary end points of death, MI or urgent revascularization were reduced to a great extent in patients receiving stenting plus abciximab as compared to angioplasty or acbiximab alone group. It has been established that abciximab and tirofiban can be used successfully in patients with peripheral arterial occlusion disease and arterial thrombosis.[64]
GP IIb/IIIa inhibitors in acute myocardial infarction
The majority of trials previously mentioned included a small number of patients with acute myocardial infarction (AMI). Until recently, overriding concern about the potential for intracranial hemorrhage induced by GP IIb/IIIa inhibition coupled with heparin, aspirin and thrombolytic therapy has precluded the large-scale investigation of GP IIb/IIIa antagonists in acute MI.[43],[44],[45],[61],[65],[66],[67],[68] Regarding the utility of GP IIb/IIIa inhibition with direct angioplasty, the RAPPORT (Reopro in acute myocardial infarction and primary PTCA organization and Randomized Trial) showed a significant reduction in the rates of urgent TVR, particularly during the first seven days.[8],[67] The Controlled Abciximab and Device Investigation to Lower Late angioplasty Complication (CADILLAC) trial suggested benefit of abciximab with both primary PTCA and primary stenting but no additional benefit of the combined use of abciximab and stents.[68] Another one, the Abciximab before Direct angioplasty and stenting in Myocardial Infarction regarding Acute and Long term follow-up (ADMIRAL) trial is also looking at the long term effects of abciximab and primary stenting.
GP IIb/IIIa inhibitors in unstable angina or non Q wave MI
GP IIb/IIIa receptor inhibitors are beneficial in unstable angina/ non-ST elevation MI.[69] Four large, randomized, placebo controlled trials evaluated parenteral GP IIb/IIIa antagonists in this syndrome. These included PRISM (Platelet Receptors inhibition in Ischemic Syndrome Management) trial, PRISM-PLUS (Platelet Receptors inhibition in Ischemic Syndrome Management in Patients Limited by Unstable signs and Symptoms) trial, PARAGON (Platelet IIb/IIIa Antagonism for the Reduction of Acute coronary syndrome events in a Global Organization Network) trial and PURSUIT (Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor SUppression using Integrilin [eptifibatide] Therapy) trial. The PRISM trial randomized patients with unstable angina/non-ST elevation MI to intravenous heparin or intravenous tirofiban for 48 h.[14] It showed a composite endpoint reduction in favor of tirofiban.[65],[70] The PRISM-PLUS trail was designed to assess whether tirofiban with heparin was better than either drug alone in the management of a similar group of patients as the PRISM trial. The tirofiban arm was terminated prematurely owing to excess mortality. However, combination of tirofiban and heparin produced highly significant reduction in 7 day composite endpoint (death, MI or refractory angina). In the PARAGON trial, another peptide GP IIb/IIIa antagonist lamifiban, in low and high dose was compared, with or without heparin. No significant benefit was however obtained in these trials.[66] The PURSUIT trial is by far the largest trial of GP IIb/IIIa therapy with 10948 patients showing eptifibatide to produce significant reduction in incidences of death or MI at 30 days in those undergoing PTCA.[67]
However, the main disadvantages of the use of GP IIb/IIIa inhibitors are an increased tendency to bleeding, thrombocytopenia and perhaps its cost as well.[71] The determination of an appropriate degree of GP IIb/IIIa blockade with agents that will be both effective and safe is perhaps the greatest challenge in the development of oral agents. The other major challenge in the development of oral antagonists will be the nature of the pharmacokinetic and pharmacodynamic variability that they display in patients.
To conclude, the GP IIb/IIIa receptor is a unique target in cardiology
for the prevention of restenosis. Various clinical trials have convincingly
established that GP IIb/IIIa receptor antagonists produce a significant
reduction of death, non-fatal myocardial infarction, emergency CABG or
PTCA, stent or balloon pump insertion for refractory angina. More comparative
studies are still required to prove the efficacy and safety of these
drugs.
REFERENCES
| 1. | Davies MJ. Pathology of arterial thrombosis. Br Med Bull 1994;50:789-802. Back to cited text no. 1 [PUBMED] |
| 2. | Brogan GX Jr. Bench to bedside: pathophysiology of acute coronary syndromes and implications for therapy. Acad Emerg Med 2002;9:1029-44. Back to cited text no. 2 [PUBMED] [FULLTEXT] |
| 3. | Ridker PM, Manson JE, Gaziano JM, Buring JE, Hennekens CH. Low dose aspirin therapy for chronic stable angina. A randomized, placebo controlled clinical trial. Ann Intern Med 1991;114:835-9. Back to cited text no. 3 [PUBMED] |
| 4. | Almony GT, Lefkovits J, Topol EJ. Antiplatelet and anticoagulant use after myocardial infarction. Clin Cardiol 1996;19:357-65. Back to cited text no. 4 [PUBMED] |
| 5. | Zed PJ, Tisdale JE, Borzak S. Low-molecular-weight heparins in the management of acute coronary syndromes. Arch Intern Med 1999;159:1849-57. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
| 6. | Hass WK, Easton JD, Adams HP Jr, Pryse-Phillips W, Molony BA, Anderson S, et al. A randomized trial comparing ticlopidine hydrochloride with aspirin for the prevention of stroke in high risk patients. N Engl J Med 1989;321:501-7. Back to cited text no. 6 |
| 7. | Gent M, Blakely JA, Easton JD, Ellis DJ, Hachinski VC, Harbison JW, et al. The Canadian American Ticlopidine Study (CATS) in thromboembolic stroke. Lancet 1989;1:1215-20. Back to cited text no. 7 |
| 8. | Brodison A, Katira R, More RS, Chauhan A. Antiplatelet use in interventional cardiology. Postgrad Med J 2000;76:70-9. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Lefkovits J, Plow EF, Topol EJ. Platelet glycoprotein IIb/IIIa receptors in cardiovascular medicine. N Engl J Med 1995;332:1553-9. Back to cited text no. 9 [PUBMED] [FULLTEXT] |
| 10. | Scarborough RM, Kleiman NS, Phillips DR. Platelet glycoprotein IIb/IIIa antagonists. What are the relevant issues concerning their pharmacology and clinical use? Circulation 1999;100:437-44. Back to cited text no. 10 [PUBMED] [FULLTEXT] |
| 11. | Phillips DR, Charo IF, Scarborough RM. GP IIb/IIIa. The responsive integrin. Cell 1991;65:359-62. Back to cited text no. 11 [PUBMED] |
| 12. | Coller BS, Scudder LE, Beer J, Gold HK, Folts JD, Cavagnaro J, et al. Monoclonal antibodies to platelet glycoprotein IIb/IIIa as antithrombotic agents. Ann N Y Acad Sci 1991;614:193-213. Back to cited text no. 12 |
| 13. | Bhatt DL, Topol EJ. Current role of platelet glycoprotein IIb/IIIa inhibitors in acute coronary syndromes. JAMA 2000;284:1549-58. Back to cited text no. 13 [PUBMED] [FULLTEXT] |
| 14. | Ruggeri ZM, Dent JA, Saldivar E. Contribution of distinct adhesive interactions to platelet aggregation in flowing blood. Blood 1999;94:172-8. Back to cited text no. 14 [PUBMED] [FULLTEXT] |
| 15. | Ruggeri ZM. Old concepts and new developments in the study of platelet aggregation. J Clin Invest 2000;105:699-701. Back to cited text no. 15 [PUBMED] [FULLTEXT] |
| 16. | Poncz M, Eisman R, Heidenreich R, Silver SM, Vilaire G, Surrey S, et al. Structure of the platelet membrane glycoprotein IIb: homology to the alpha subunits of the vitronectin and fibronectin membrane receptors. J Biol Chem 1987;262:8476-82. Back to cited text no. 16 |
| 17. | Kunicki TJ, Pidard D, Rosa JP, Nurden AT. The formation of Ca++-dependent complexes of platelet membrane glycoproteins IIb and IIIa in solution as determined by crossed immunoelectrophoresis. Blood 1981;58:268-78. Back to cited text no. 17 [PUBMED] |
| 18. | Fujimura K, Phillips DR. Calcium cation regulation of glycoprotein IIb-IIIa complex formation in platelet plasma membranes. J Biol Chem 1983;258:10247-52. Back to cited text no. 18 [PUBMED] [FULLTEXT] |
| 19. | Madan M, Berkowitz SD, Tcheng JE. Glycoprotein IIb/IIIa integrin blockade. Circulation 1998;98:2629-35. Back to cited text no. 19 [PUBMED] [FULLTEXT] |
| 20. | Kieffer N, Fitzgerald LA, Wolf D, Cheresh DA, Phillips DR. Adhesive properties of the beta 3 integrins: comparison of GP IIb/IIIa and the vitronectin receptor individually expressed in human melanoma cells. J Cell Biol 1991;113:451-61 Back to cited text no. 20 [PUBMED] [FULLTEXT] |
| 21. | Byzova TV, Plow EF. Networking in the hemostatic system. Integrin alphaiibbeta3 binds prothrombin and influences its activation. J Biol Chem 1997;272:27183-8. Back to cited text no. 21 [PUBMED] [FULLTEXT] |
| 22. | Gogstad GO, Brosstad F, Krutnes MB, Hagen I, Solum NO. Fibrinogen-binding properties of the human platelet glycoprotein IIb-IIIa complex: a study using crossed-radioimmunoelectrophoresis. Blood 1982;60:663-71. Back to cited text no. 22 [PUBMED] |
| 23. | Plow EF, Ginsberg MH. Cellular adhesion: GPIIb-IIIa as a prototypic adhesion receptor. Prog Hemost Thromb 1989;9:117-56. Back to cited text no. 23 [PUBMED] |
| 24. | Parise LV, Phillips DR. Reconstitution of the purified platelet fibrinogen receptor: fibrinogen binding properties of the glycoprotein IIb-IIIa complex. J Biol Chem 1985;260:10698-707. Back to cited text no. 24 [PUBMED] [FULLTEXT] |
| 25. | Plow EF, Ginsberg MH. Specific and saturable binding of plasma fibronectin to thrombin-stimulated platelets. J Biol Chem 1981;256:9477-82. Back to cited text no. 25 [PUBMED] [FULLTEXT] |
| 26. | Plow EF, Srouji AH, Meyer D, Marguerie G, Ginsberg MH. Evidence that three adhesive proteins interact with a common recognition site on activated platelets. J Biol Chem 1984;259:5388-91. Back to cited text no. 26 [PUBMED] [FULLTEXT] |
| 27. | Coller BS. GP IIb/IIIa antagonists: pathophysiologic and therapeutic insights from studies of c7E3 Fab. Thromb Haemost 1997;78:730-5. Back to cited text no. 27 [PUBMED] |
| 28. | Ruoslahti E, Pierschbacher MD. Arg-Gly-Asp: a versatile cell recognition signal. Cell 1986;44:517-8. Back to cited text no. 28 [PUBMED] |
| 29. | Holmback K, Danton MJ, Suh TT, Daugherty CC, Degen JL. Impaired platelet aggregation and sustained bleeding in mice lacking the fibrinogen motif bound by integrin IIb 3. EMBO J 1996;15:5760-71. Back to cited text no. 29 [PUBMED] |
| 30. | Kloczewiak M, Timmons S, Lukas TJ, Hawiger J. Platelet receptor recognition site on human fibrinogen: synthesis and structure-function relationship of peptides corresponding to the carboxy-terminal segment of the gamma chain. Biochemistry 1984;23:1767-74. Back to cited text no. 30 [PUBMED] |
| 31. | Weisel JW, Nagaswami C, Vilaire G, Bennett JS. Examination of the platelet membrane glycoprotein IIb/IIIa complex and its interaction with fibrinogen and other ligands by electron microscopy. J Biol Chem 1992;267:16637-43. Back to cited text no. 31 [PUBMED] [FULLTEXT] |
| 32. | Plow EF, Marguerie G, Ginsberg M. Fibrinogen, fibrinogen receptors, and the peptides that inhibit these interactions. Biochem Pharmacol 1987;36:4035-40. Back to cited text no. 32 [PUBMED] |
| 33. | Calvete JJ. Clues for understanding the structure and function of a prototypic human integrin: the platelet glycoprotein IIb/IIIa complex. Thromb Haemost 1994;72:1-15. Back to cited text no. 33 [PUBMED] |
| 34. | Wencel-Drake JD, Plow EF, Kunicki TJ, Woods VL, Keller DM, Ginsberg MH. Localization of internal pools of membrane glycoproteins involved in platelet adhesive responses. Am J Pathol 1986;124:324-34. Back to cited text no. 34 [PUBMED] |
| 35. | Topol EJ. Toward a new frontier in myocardial reperfusion therapy: emerging platelet preeminence. Circulation 1998;97:211-8. Back to cited text no. 35 [PUBMED] [FULLTEXT] |
| 36. | Mousa SA, Bennett JS. Platelets in health and disease: platelet GP IIb/IIIa structure and function: recent advances in antiplatelet therapy. Drugs Future 1996;21:1141-54. Back to cited text no. 36 |
| 37. | Cook NS, Kottirsch G, Zerwes H-G. Platelet glycoprotein IIb/IIIa antagonists. Drugs Future 1994;19:135-59. Back to cited text no. 37 |
| 38. | Zablocki JA, Nicholson NS, Feigen LP. Fibrinogen receptor antagonists. Exp Opin Invest Drugs 1994;3:437-48. Back to cited text no. 38 |
| 39. | Lefkovits J, Topol EJ. Platelet glycoprotein IIb/IIIa receptor antagonists in coronary artery disease. Eur Heart J 1996;17:9-18. Back to cited text no. 39 |
| 40. | Paul W, Armstrong MD. Unsticking platelets : the role of Glycoprotein IIb/IIIa receptor blockade. Canad Med Assoc J 1999;161:1423-6. Back to cited text no. 40 |
| 41. | Kleiman NS, Raizer AE, Jordan R, Wang AL, Norton D, Mace KF, et al. Differential inhibition of platelet aggregation induce by adenosine diphosphate or a thrombin receptor-activating peptide in patients treated with chimeric 7E3 Fab: implications for inhibition of the internal pool of GP IIb/IIIa receptors. J Am Coll Cardiol 1995;26:1665-71. Back to cited text no. 41 |
| 42. | Coller BS, Peerschke EI, Scudder LE, Sullivan CA. A murine monoclonal antibody that completely blocks the binding of fibrinogen to platelets produces a thrombasthenic -like state in normal platelets and binds to glycoprotein IIb and /or IIIa. J Clin Invest 1983;72:325-38. Back to cited text no. 42 [PUBMED] |
| 43. | EPIC investigators. Use of a monoclonal antibody directed against the platelet glycoprotein IIb/IIIa receptor in high-risk cornary angioplasty. N Engl J Med 1994;330:956-61. Back to cited text no. 43 |
| 44. | The CAPTURE Investigators. Randomized placebo-controlled trial of abciximab before and during coronary intervention in refractory unstable angina: the CAPTURE study. Lancet 1997;349:1429-35. Back to cited text no. 44 |
| 45. | EPILOG investigators. Platelet glycoprotein IIb/IIIa receptors blockade and low-dose heparin during percutaneous coronary revascularisation. N Engl. J Med 1997;336:1689-96. Back to cited text no. 45 |
| 46. | Barker PL, Bullens S, Buntina S, Burdick DJ, Chan KS, Deisher T, et al. Cyclic RGD peptide analogues as antiplatelet antithrombotics. J Med Chem 1992;35:2040-8. Back to cited text no. 46 |
| 47. | Mousa SA, Bozarth JM, Lorelli W, Forsythe MS, Thoolen MJ, Slee AM, et al. Antiplatelet efficacy of XV 459, a novel nonpeptide GP IIb/IIIa antagonist; comparative platelet binding profile with c7E3. J Pharmacol Exp Ther 1998;256: 1277-84. Back to cited text no. 47 |
| 48. | Cook JJ, Sitko GR, Holahan MA, Stranieri MT, Glass JD, Askew BC, et al. Nonpeptide glycoprotein IIb/IIIa inhibition. 15. Antithrombotic efficacy of L-738,167, a long acting GP IIb/IIIa antagonist, correlates with inhibition of adenosine diphosphate induced platelet aggregation but not with bleeding time prolongation. J Pharmacol Exp Ther 1997;281:677-89. Back to cited text no. 48 |
| 49. | Frelinger AL 3rd, Furman MI, Krueger LA, Barnard MR, Michelson DA. Dissociation of glycoprotein IIb/IIIa antagonists from platelets does not result in fibrinogen binding or platelet aggregation. Circulation 2001;104:1374-80. Back to cited text no. 49 |
| 50. | Serebruany VL, Malinin AI, O'connon CM, Gurbel PA. Effects of roxifiban on platelet aggregation and major receptor expression in patients with coronary artery disease for the Roxifiban Oral Compound Kinetics Evaluation Trial-I (ROCKET-I Platelet Substudy). Am Heart J 2003;146:91-8. Back to cited text no. 50 |
| 51. | Mascelli MA, Lance ET, Damaraju L, Wagner CL, Weisman HF, Jordan RE. Pharmacodynamic profile of short-term abciximab treatment demonstrates prolonged platelet inhibition with gradual recovery from GP IIb/IIIa receptor blockade. Circulation 1998;97:1680-8. Back to cited text no. 51 [PUBMED] [FULLTEXT] |
| 52. | Tcheng JE, Ellis SG, George BS, Kereiakes DJ, Kleiman NS, Talley JD, et al. Pharmacodynamics of chimeric glycoprotein IIb/IIIa integrin antiplatelet antibody Fab 7E3 in high-risk coronary angioplasty. Circulation 1994;90:1757-64. Back to cited text no. 52 |
| 53. | Pang JT, Fort S, Della Siega A, Cohen EA. Emergency coronary artery bypass surgery in the era of glycoprotein IIb/IIIa receptor antagonist use. J Card Surg 2002;17:425-31. Back to cited text no. 53 [PUBMED] |
| 54. | Tam SH, Sassoli PM, Jordan RE, Nakada MT. Abciximab (ReoPro, Chimeric 7E3 Fab) demonstrates equivalent affinity and functional blockade of glycoprotein IIb/IIIa and v 3 integrins. Circulation 1998;98:1085-91. Back to cited text no. 54 [PUBMED] [FULLTEXT] |
| 55. | Simon DI, Xu H, Ortlepp S, Rogers C, Rao NK. 7E3 monoclonal antibody directed against the platelet glycoprotein IIb/IIIa cross-reacts with the leukocyte integrin Mac-1 and blocks adhesion to fibrinogen and ICAM-1. Arterioscler Thromb Vasc Biol 1997;17:528-35. Back to cited text no. 55 [PUBMED] [FULLTEXT] |
| 56. | Tcheng JE, Kereiakes DJ, Lincoff AM, George BS, Kleiman NS, Sane DC, et al. Abciximab readministration: results of the ReoPro Readministration Registry. Circulation 2001;104:870-5. Back to cited text no. 56 |
| 57. | Curtin R, Fitzgerald DJ. Pharmacogenetics of antiplatelet drugs. Scientific World Journal 2002;2:791-800. Back to cited text no. 57 [PUBMED] |
| 58. | Nannizzi-Alaimo L, Alves VL, Phillips DR. Inhibitory effects of glycoprotein IIb/IIIa antagonists and aspirin on the release of soluble CD40 ligand during platelet stimulation. Circulation 2003;107:1123-8. Back to cited text no. 58 [PUBMED] [FULLTEXT] |
| 59. | Ryan TJ, Faxon DP, Gunnar RM. Guidelines for percutaneuous transluminal coronary angioplasty: a report of the American College of Cardiology/American Heart Association task force on assessment of diagnostic and therapeutic cardiovascular procedures. Circulation 1998;278:486-502. Back to cited text no. 59 |
| 60. | Bednar B, Cook JJ, Holahan MA, Cunningham ME, Jumes PA, Bednar RA, et al. Fibrinogen receptor antagonist-induced thrombocytopenia in chimpanzee and rhesus monkey associated with preexisting drug-dependent antibodies to platelet glycoprotein IIb/IIIa. Blood 1999;94:587-99. Back to cited text no. 60 |
| 61. | The RESTORE investigators. Effects of platelet glycoprotein IIb/IIIa blockade with tirofiban on adverse cardiac events in patients with unstable angina or acute myocardial infarction undergoing coronary angioplasty. Circulation 1997; 96:1445-53. Back to cited text no. 61 [PUBMED] [FULLTEXT] |
| 62. | The IMPACT-II investigators. Randomized placebo-controlled trial of the effect of eptifibatide on complications of percutaneous coronary intervention: IMPACT-II. Lancet 1997;349:1422-8. Back to cited text no. 62 |
| 63. | The EPISTENT investigators. Randomised placebo-controlled and balloon-angioplasty-controlled trial to assess safety of coronary stenting with the use of platelet glycoprotein IIb/IIIa blockade. Lancet 1998;352:87-92. Back to cited text no. 63 [PUBMED] [FULLTEXT] |
| 64. | Schweizer J, Kirch W, Koch R, Muller A, Hellner G, Forkmann L. Use of abciximab and tirofiban in patients with peripheral arterial occlusive disease and arterial thrombosis. Angiology 2003;54:155-61. Back to cited text no. 64 [PUBMED] |
| 65. | Ferguson JJ. Meeting highlights: 46th annual scientific sessions of the American College of Cardiology. Circulation 1997;96:367-71. Back to cited text no. 65 [PUBMED] [FULLTEXT] |
| 66. | The PARAGON investigators. International, randomized, controlled trial of lamifiban ( a platelet glycoprotein IIb/IIIa inhibitor), heparin or both in unstable angina. Circulation 1998;97:2386-95. Back to cited text no. 66 [PUBMED] [FULLTEXT] |
| 67. | The PERSUIT trial investigators. Inhibition of platelet glycoprotein IIb/IIIa with eptifibatide in patients with acute coronary syndromes. N Engl J Med 1998; 339:436-43. Back to cited text no. 67 |
| 68. | Stone GW. Stenting in acute myocardial infarction. Observational studies and randomized trials N 1998. J Invasive Cardiol 1998;10:16-26. Back to cited text no. 68 |
| 69. | Cannon CP. Small molecule glycoprotein IIb/IIIa receptor inhibitors as upstream therapy in acute coronary syndromes: insights from the TACTICS-TIMI 18 trial. J Am Coll Cardiol 2003;41:43-8. Back to cited text no. 69 |
| 70. | The PRISM investigators. A comparison of aspirin plus tirofiban with aspirin plus heparin for unstable angina. N Engl J Med 1998;338:1498-505. Back to cited text no. 70 |
| 71. | Goklaney AK, Murphy JD, Hillegass WB. Abciximab therapy in percutaneous intervetion:economic issues in the United States. Eur Heart J 1998;19:52-8. Back to cited text no. 71 |
Copyright 2004 - Indian Journal of Pharmacology
The following images related to this document are available:
Photo images
[ph04049f2.jpg]
[ph04049t1.jpg]
[ph04049f3.jpg]
[ph04049f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}