
|
Indian Journal of Pharmacology
Medknow Publications on behalf of Indian Pharmacological Society
ISSN: 0253-7613 EISSN: 1998-3751
Vol. 36, Num. 3, 2004, pp. 183-185
|
Indian Journal of Pharmacology, Vol. 36, No. 3, June, 2004, pp. 183-185
Case Report
Risperidone-induced tardive movements in young adult patients
Mendhekar DN
Department of Psychiatry, G. B. Pant Hospital, New Delhi - 110002
Correspondence Address:Department of Psychiatry, G. B. Pant Hospital,
New Delhi - 110002 dnmendhekar@vsnl.net
Code Number: ph04065
Risperidone, a benzisoxazole compound, was the first of the new antipsychotic drugs to be introduced. Persistent abnormal movements such as tardive dyskinesia and dystonia are not common side effects associated with risperidone therapy. The low rate of emergent persistent dyskinesia in the geriatric population while on risperidone suggests that it is probably associated with a very low incidence of tardive movements in younger patients.[1] Here, we report a series of four cases with risperidone-induced tardive dyskinesia and dystonia and discuss their management.
CASE
REPORTS
Case A
A 21-year-old male engineering student presented with a four-year history of paranoid schizophrenia. Illness had insidious onset with multiple exacerbations. Initially, he was treated with trifluperazine and had marked improvement but he discontinued medication after two weeks. There was an exacerbation of symptoms after one year of drug naïve period. At that time he was treated with risperidone, which was gradually increased from 2 mg to 6 mg/day over a period of 4 weeks. This time too the patient showed improvement and risperidone 4 mg was continued for the next two years as maintenance therapy. After two years of continuous treatment with risperidone, the patient showed choreoathetoid movements of both hands, right more than the left, characterized by pulling sensations (as if he was pulling his pant upwards). To prevent these movements, he would clench his hands tightly and would keep them in his pockets. MRI head showed no abnormality. The patient was switched to clozapine (12.5 mg/day), gradually increasing to 75 mg/day but he could not tolerate the sedative effect. Hence, clozapine was decreased to 25 mg/day and tetrabenazine 25 mg/day was added and gradually increased to 75 mg/day. Within 4 months the patient showed complete recovery from dyskinetic movement. Case B
A 24-year-old male presented with a three-year history of paranoid schizophrenia. He was started on risperidone 2 mg/day and it was increased to 4 mg/day over a period of 4 weeks with remarkable improvement. With 4 months of risperidone therapy, the patient was noticed to have bilateral rhythmic movements of both fingers and thumbs, and oromandibular dystonia with difficulty in speaking and eating. A neurological opinion was sought and a diagnosis of drug-induced tardive dyskinesia and dystonia was opined. A trial of intravenous promethazine 50 mg did not show any change in both movements. Risperidone was replaced by olanzapine 5 mg/day which was later increased to 12.5 mg/day over a period of 6 weeks, on which the patient showed significant improvement in abnormal movements (including dystonia) without any relapse in psychotic symptoms. There was no past history of exposure to conventional antipsychotics at any time. Case C
An 18-year-old girl presented with history suggestive of psychosis of 4 years duration. Six months after the onset of psychiatric illness she started having attacks of generalized tonic-clonic (GTC) seizure. The frequency of seizure varied from once in 10 days to once in 20 days. She did not receive any treatment for both the illnesses till one year back. Her personal history revealed that she was a mouth breather since childhood. Initially, she was put on phenytoin 300 mg/day. Though her seizures were controlled, she continued to exhibit psychotic symptoms hence she was referred to a psychiatrist. In view of the occurrence of both psychosis and seizure, phenytoin, which she had been taking for the last 4 months, was stopped and carbamazepine 800 mg/day was started with hematological monitoring. There was no fresh attack of seizure but her psychotic symptoms persisted. Hence, risperidone 1mg/day was added and increased to 2 mg/day over a period of 1 month. After 3 months on this combination, she exhibited dyskinetic movements in the form of pill-rolling movements of the fingers and oromandibular dystonia (widening of mouth) with difficulty in speaking and eating. Risperidone was stopped immediately and parenteral promethazine was given without any improvement. Due to the persistence of psychotic symptoms and the appearance of abnormal movements, olanzapine 2.5 mg/day was added and it was increased to 10 mg/day over a period of 4 weeks. Within 10 weeks she showed remarkable improvement in dystonia and psychotic symptoms but her hand′s dyskinetic movements remained the same. However, olanzapine was continued for 6 months along with carbamazepine. Case D
A 20-year-old male with sub-average intelligence and a past history of seizure disorder presented with a five-year duration of severe behavioral problems. He was on thioridazine 100 mg/day for the last 3 months. He was a mouth breather since childhood. He was given risperidone 2 mg/day and clonazepam 1 mg/day with mild improvement. After two months, oromandibular dystonia, with difficulty in speaking and eating was noticed. Risperidone was stopped and olanzapine 5 mg/day was started and gradually increased to 15 mg/day. The patient showed mild improvement in psychosis but oro-mandibular dystonia persisted. Later olanzapine was stopped and clozapine 12.5 mg/day was started. This was gradually increased to 100 mg/day. The patient could not tolerate the sedative effect hence clozapine was stopped. The patient did not turn up for one year thereafter. On his subsequent visit it was observed that abnormal movement persisted along with his behavioral problems. He was given carbamazepine 1000 mg/day and had only mild improvement in both his behavioral problems and his abnormal movements. Subsequently, he was given trihexyphenidyl 2 mg/day, which was gradually increased to 10 mg/day in divided doses. The patient showed partial improvement in oromandibular dystonia and was able to eat and speak better than before. DISCUSSION
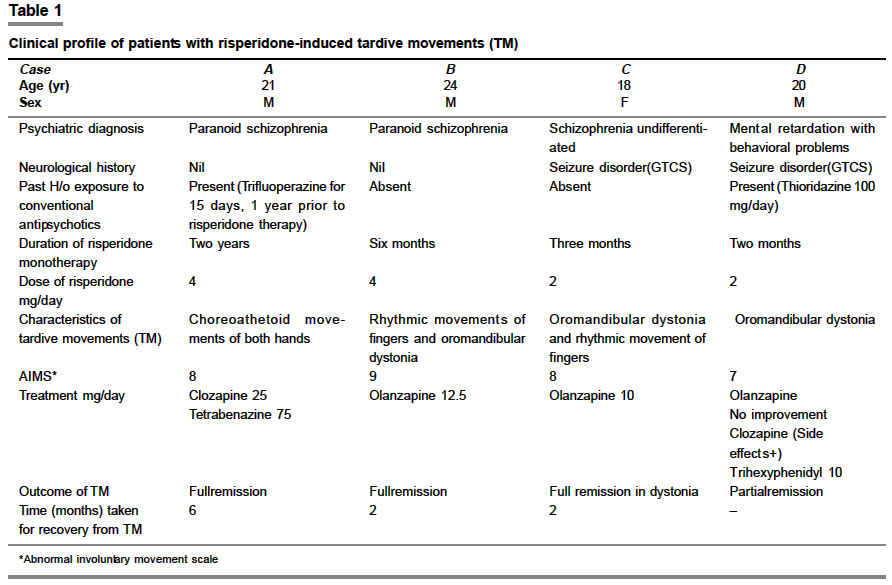
The clinical profile of all patients are tabulated for easy comparison [Table
- 1]. All these patients discussed had received risperidone. There was no past history of dyskinetic movements, and their temporal relationship definitely suggests risperidone-induced tardive dyskinesia. These cases have fulfilled the DSM IV[2] diagnostic criteria of Tardive dyskinesia and dystonia except Case D where the duration of exposure to risperidone was only for two months (instead of 3 months) when dystonia emerged. However, it persisted for more than a year. In a previous report dyskinesia appeared in 3 cases within 3 months of risperidone therapy.[3] The same study observed no new cases of dyskinesia after 3 months of risperidone therapy. In the present study half the sample was exposed to conventional antipsychotics at least 2 months prior to the initiation of risperidone therapy and two cases had history of central nervous system (CNS) dysfunction in the form of seizure disorder. One of the striking features of this study was that those who had history of seizure disorder developed tardive movements within two to three months of risperidone therapy and at low doses (1-2 mg/day) in comparison to cases with functional psychosis. Apart from tardive dyskinesia, the majority of our sample showed typical oromandibular dystonia. Personal history of mouth breathing may be an incidental finding.
Clozapine has been used in the management of tardive dyskinesia and
tardive dystonia with dystonic features being more responsive than dyskinetic
ones.[4] Olanzapine has also
been found to be effective in the management of tardive movement disorder.[5] Tetrabenazine,
usually in the range of 25-150 mg/day has been found effective in a proportion
of patients.[6] Most data
indicate that long-term treatment with anticholinergics either does not
help or may actually worsen movements and their discontinuation may be
helpful in up to 60% of patients.[7] An
important exception is tardive dystonia, which may improve markedly with
moderate to high doses (20 mg/day or higher) of anticholinergics such
as trihexiphenidyl.[8]
In our case series, the first patient responded to a combination of low
doses of clozapine and tetrabenazine, the second and third patients to
olanzapine and the fourth patient had partial improvement with a high dose
of trihexiphenidyl. In our sample, two patients (Cases C and D) with history
of childhood seizure did not show appreciable improvement, indicating that
preexisting CNS abnormality may be a poor prognostic factor for patients
with tardive movements. We tried clozapine in two cases (Cases A and D)
but these cases were sensitive to the sedative effect of clozapine.
In conclusion, irrespective of the safety profile associated with newer
atypical antipsychotic drugs, a clinician must be on the lookout for
rare side effects.
REFERENCES
| 1. | Jeste DV, Okamato A, Napolitano J, Kane JM, Martinez RA. Low incidence of persistent tardive dyskinesia in elderly patients with dementia treated with risperidone. Am J Psychiatry 2000;157:1150-5. Back to cited text no. 1 |
| 2. | American Psychiatric Association. Tardive dyskinesia In: Diagnostic and statistical manual of mental disorders. 4th ed. Washington: American Psychiatric Association; 1994. Back to cited text no. 2 |
| 3. | Jeste DV, Lacro JP, Bailey A, Rockwell E, Harris MJ, Caligiuri MP. Low incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47:716-9. Back to cited text no. 3 [PUBMED] |
| 4. | Caroff SN, Mann SC, Campbell EC, Sullivan KA. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry 2002;63(Suppl 4):12-9. Back to cited text no. 4 [PUBMED] |
| 5. | ALMENDA OP. Olanzapine for the treatment of tardive dyskinesia. J Clin Psychiatry 1998;59:380-1. Back to cited text no. 5 |
| 6. | Jankovic J, Beach J. Long-term effects of tetrabenazine in hyperkinetic movement disorders. Neurology 1997;48:358-62. Back to cited text no. 6 [PUBMED] |
| 7. | Sachdeva PS. The current status of tardive dyskinesia. Aust N Z J Psychiatry 2000;34:355-69. Back to cited text no. 7 |
| 8. | Libermann JA, Saltz BL, Johns CA, Pollack S, Borenstein M, Kane J. The effects of clozapine on tardive dyskinesia. Br J Psychiatry 1991;158:503-10. Back to cited text no. 8 |
Copyright 2004 - Indian Journal of Pharmacology
The following images related to this document are available:
Photo images
[ph04065t1.jpg]
|

{kind=link}