 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
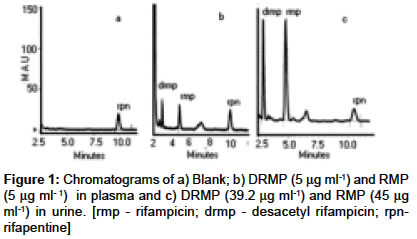
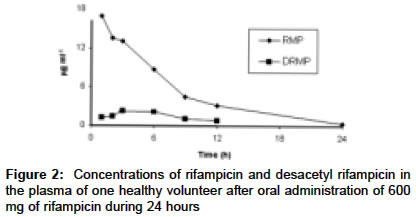
Indian Journal of Pharmacology, Vol. 36, No. 4, August, 2004, pp. 231-233 Research Paper A validated high-performance liquid chromatography method for the determination of rifampicin and desacetyl rifampicin in plasma and urine Hemanth Kumar AK, Chandra I, Geetha R, Chelvi KS, Lalitha V, Prema G Tuberculosis Research Centre (ICMR), Chennai Code Number: ph04076 ABSTRACT OBJECTIVE: To standardize a high-performance liquid chromatography (HPLC) method for the determination of rifampicin (RMP) and its major metabolite desacetyl rifampicin (DRMP) in plasma and urine. MATERIAL AND METHODS: A simple, specific and sensitive HPLC method was developed for the determination of RMP and DRMP in plasma and urine. Separation in both was achieved by reverse-phase chromatography on a C18 column with a mobile phase composition of 0.05 M phosphate buffer: acetonitrile (55:45 v/v) at 254 nm. RESULTS: The retention times of DRMP, RMP and Rifapentine (RPN), the internal standard were 2.9, 4.8 and 10.5 min respectively. The assay was linear from 0.25 to 15.0 g ml-1 for plasma and 2.5 to 80.0 g ml-1 for urine. Both intra-day and inter-day accuracy and precision data showed good reproducibility. CONCLUSION: The HPLC method described is sensitive, selective and linear for the wide range of concentrations for RMP and DRMP in plasma and urine. Thus, the method developed is well suited for the pharmacokinetic studies. Keywords: Rifampin, rifamycin, HPLC INTRODUCTION Rifampicin (3-[4-methyl piperazinyl-iminomethyl] rifamycin SV; rifampin), a semi-synthetic drug, is the key sterilizing component of highly effective short course antituberculous regimens and has a unique role in the killing of semi-dormant tubercle bacilli.[1] Very few HPLC methods have been developed for the quantification of RMP and its metabolite, DRMP in the plasma[2],[3],[4] and urine.[5],[6],[7],[8] These HPLC methods involve tedious procedures which are time-consuming. Also, the microbiological assay does not permit separate determination of RMP and DRMP in biological fluids.[9] Therefore, our aim was to standardize a method for the determination of RMP and DRMP in biological fluids by modifying certain experimental conditions of the existing methods to enable good resolution between RMP and DRMP peaks with shorter run time. After a number of trials using different combinations, we arrived at the present mobile phase and wavelength. This method is modified from the thin-layer chromatography method[10] which outperformed all the HPLC procedures in its precision when our laboratory participated in the international network initiated by WHO Global TB program for evaluating the RMP bioavailability of Fixed Dose Combinations (FDC).[11] MATERIAL AND METHODS Chemicals: Pure RMP standard was obtained from Sigma Chemicals Company (St.Louis, Mo, USA). DRMP and RPN were gifted by Dr. G. A. Ellard, (BMRC, London), Acetonitrile, chloroform and methanol used were of HPLC grade obtained from Merck (Mumbai, India). The chemicals, potassium dihydrogen orthophosphate, disodium hydrogen phosphate, citric acid and ascorbic acid were of analytical grade. Deionized water was processed through a Milli-Q water purification system (Millipore, USA). Chromatographic system: The HPLC system (Shimadzu Corporation, Kyoto, Japan) consisted of two pumps (LC-10ATvp), diode array detector (SPD-M10Avp) at 254 nm and system controller (SCL-10Avp). A rheodyne manual injector (Rheodyne, Cotati, CA, USA) attached with a 20 m sample loop was used for loading the sample. ClassVP-LC workstation was used for data collection and acquisition. The analytical column was a LUNA C18, 250 X 4.6 mm ID, 5 m particle size (Phenomenex, Torrance, CA, USA) protected by security guard column, 4-mm L X 3.0-mm ID (Lichrospher 100 RP-18e, Merck, Germany). The mobile phase was 0.05 M potassium dihydrogen phosphate buffer (pH 2.6): acetonitrile (55:45 v/v) with a flow rate of 1.2 ml min-1 at ambient temperature. The chromatogram was run for 12 min. Unknown concentrations were derived from the linear regression analysis of the peak height ratios (analyte/internal standard) Vs. concentration curve. Linearity was verified using estimates of correlation coefficient (r). Preparation of standard solution: A stock standard solution of RMP and DRMP was prepared by dissolving 10 mg of each in 10 ml methanol containing 0.5 mg/ml of ascorbic acid. A stock solution of RPN was prepared by dissolving 12.5 mg in 10 ml acetonitrile. The combined working standards of RMP and DRMP in concentrations ranging from 0.25-15 mg ml-1 were prepared by appropriate dilution with pooled plasma. The urine standards ranging from 2.5-80 mg ml-1 were prepared in pooled urine. The internal standard was diluted in acetonitrile to give a concentration of 1.25 mg/10 ml for usage in the plasma assay. The stock solution of 12.5 mg/10 ml as such was used in the urine assay. Sample preparation: An aliquot of 200 ml of blank plasma, standard or test samples was pipetted into an eppendorf′s tube of 1.5 ml capacity which contained 20 ml of 1.25 mg/10 ml of RPN. Acetonitrile (300 ml) was added, vortexed for one minute and microcentrifuged at 10,000 rpm for 5 min. Then, 300 ml of the supernatant was taken into another microcentrifuge tube and vacuum dried in the HETO vacuum centrifuge (Allerod, Denmark). The residue obtained was reconstituted in 100 ml of mobile phase and 20 ml volume was injected. An aliquot of 2.0 ml of blank urine, standard or test sample was added in a tube containing 40 ml of 12.5 mg/10 ml of RPN. The contents were mixed with 1.0 ml of citrate-phosphate buffer (1.5 M, pH 7.0) and extracted with 2.0 ml chloroform by vortexing for one min. The volume of test sample taken for assay varied for the samples containing concentrations greater than 80 mg ml-1. The ratio of buffer to the volume of sample was similar (1:2) and 2.0 ml of chloroform was used uniformly for extraction. The mixture was centrifuged at 2500 rpm for 10 min. The aqueous layer was discarded and 500 ml of chloroform extract was transferred to another glass tube and evaporated at 60°C in a water bath. The residue was reconstituted in 500 ml of mobile phase and 20 ml volume was injected. RESULTS Under the chromatographic conditions described above, the two compounds, DRMP and RMP were well separated from each other as seen in the representative chromatogram [Figure - 1]. The mean retention time of DRMP, RMP and RPN was 2.9, 4.8 and 10.5 min respectively. Isoniazid, pyrazinamide (PZA) and their metabolites and ethambutol (EMB), which are often co-administered with RMP, did not interfere with the chromatograms. The calibration curves for DRMP and RMP in plasma were plotted. These curves were found to be linear over the concentration range of 0.25 to 15 mg ml-1 with correlation coefficients (r) greater than 0.9996. In urine, the curve was linear from 2.5 to 80 mg/l with r-value greater than 0.9943. The relative standard deviation (RSD) for calculated concentrations of RMP assay in plasma and urine was less than 5% except for 2.5 mg ml-1 concentration in urine. However, the RSD for DRMP was much greater ranging from 0.6 to 20.1% for plasma and 3.7 to 19.3% for urine, the greatest being for the lowest standard. The Limit of detection (LOD) and Limit of quantitation (LOQ) estimated mathematically from the standard curve equation,[12] were 0.1 and 0.25 mg ml-1 and 1.0 and 2.5 mg ml-1 for the plasma and urine assays respectively. The intra-day precision was measured by RSD of the daily mean and it was less than 3.5 % at the three control concentrations in plasma RMP and two control preparations in DRMP. The RSD of the lowest control of DRMP was 11.6%. The intra-day precision of the three control concentrations in urine was better than that of plasma for both RMP and DRMP, the RSD being less than 1.8%. The inter-day variability was highest for plasma DRMP (<11%), the next being plasma RMP (<6.4%) and much lower for urine RMP and DRMP ranging from 1.0 to 4.6%. These results suggest that reproducibility is much better for the urine assay. The overall accuracy ranged from 94 to 102 %. The recovery of RMP and DRMP was assessed by spiking known concentrations to human plasma samples containing previously determined concentrations of RMP and DRMP. This experiment was done only for plasma. The recovery ranged from 100 to 104% for RMP and 90 to 113% for DRMP. The method described was applied for the determination of RMP and DRMP in the plasma and urine of a healthy volunteer following oral administration of 600 mg of RMP. [Figure - 2] shows the pharmacokinetic profile of plasma RMP and DRMP. Rifampicin was detectable up to 24 h after the dose. In urine, both RMP and DRMP were detectable beyond 24 h (data not presented). DISCUSSION It is important to measure RMP as well as DRMP because DRMP has an antimycobacterial activity closely similar to RMP. Moreover, HPLC procedures that could efficiently separate and accurately measure both compounds were thought to be more robust and precise than those designed to measure only RMP. Lastly, it was hoped that calculated plasma and urine DRMP/RMP ratios and exploring their changes with time might uncover individual patterns in RMP desacetylation. Hence, the experimental conditions were optimized to permit good resolution between DRMP and RMP peaks with shorter run time. The mobile phase varied by changing the proportion of acetonitrile to the buffer. Increasing the proportion of acetonitrile (65%) eluted DRMP close to the solvent front while decreasing the proportion (35%) resulted in the peaks being wide apart with double the retention time and decrease in the height. The best resolution was obtained using 45% of acetonitrile. Extraction of urinary RMP and DRMP with chloroform instead of acetonitrile eliminated the contaminants and thereby prevented contamination of the column. The UV spectrum of RMP depends on the nature of the mobile phase. The wavelength set at 254 nm was compared with 215 and 340 nm. At 254 nm, less interfering peaks were observed than at 215 nm and more peak height than at 340 nm. There has been an increasing demand for a suitable method for the assay of RMP and DRMP in biological fluids of patients taking this drug. However, currently only the limited assay procedure for RMP and DRMP quantitation by HPLC are available and these involve cumbersome and time-consuming extraction procedures. Attempts were made to simplify and improve the assay methods by the use of the simple extraction procedure. Hence, the HPLC method described is sensitive, selective and linear for the wide range of concentrations for RMP and DRMP in plasma and urine. The detection limit of 1.0 mg ml-1 for urine assay enables the method to identify non-compliance with RMP therapy in tuberculosis patients. This precise and simple method utilizes a single step extraction. The chromatogram has a good resolved peak for DRMP in urine with good intra- and inter-day precision. The urinary-based approach for assessing the relative bioavailability of rifampicin in FDC antituberculosis formulations has been shown to be satisfactory.[13] The method described can be used to monitor RMP concentrations in patients who are administered rifampicin-containing regimens. ACKNOWLEDGEMENT The authors acknowledge the support and valuable suggestions provided by Dr. V. Kumaraswamy, in preparing the manuscript. We also thank Mr. B. Doraiswamy for his secretarial assistance. REFERENCES
Copyright 2004 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph04076f2.jpg] [ph04076f1.jpg] |
| |||||||||

{kind=link}
{kind=link}