 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 36, No. 6, November-December, 2004, pp. 360-362 Research Paper Comparison of the clinical efficacy of three brands of warfarin Namazi MH, Yousefi ZK, Shirazi MG, Shaykholeslami M, Vakili H, Moatamedi MR, Safi M, Forotaghe AN Department of Cardiology, Cardiovascular Research Center, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran Code Number: ph04128 ABSTRACT OBJECTIVE: To compare the clinical efficacy of three brands of warfarin.
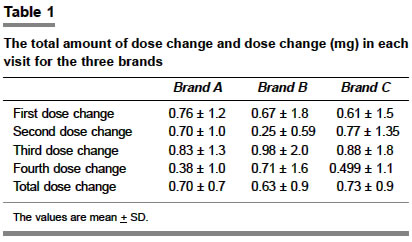
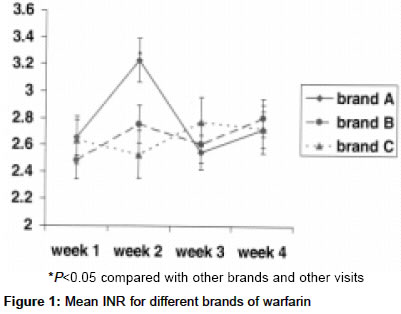
KEY WORDS: INR, oral anticoagulant, prothrombin time INTRODUCTION Warfarin is a common anticoagulant which is used in a variety of clinical settings. The drug is vital to many patients at increased risk of thromboembolic complications, and is often prescribed for patients with artificial heart valves, arrhythmias or other conditions that increase the risk of coagulation. Studies have shown the beneficial effects of warfarin administration in the prevention of stroke in patients with atrial fibrillation.[1],[2] Different formulations and brands of warfarin are available. Warfarin sodium has been added to the formulary as the generic alternative to the brand Coumadin, which is the eleventh most prescribed medication in the United States.[3] The Food and Drugs Administration of USA (FDA) has granted some products of generic warfarin an "AB" rating, indicating a therapeutic equivalence to the brand Coumadin.[4] Clinical trials have demonstrated that generic warfarin is comparable to the brand Coumadin in its effectiveness, ability to maintain stable anticoagulation, and safety.[5],[6],[7] When initiating anticoagulant therapy or when converting patients from the brand Coumadin to generic warfarin, additional monitoring of the International Normalized Ratio (INR) may be needed. In 1980, conversion from DuPont crystalline warfarin to an amorphous warfarin caused an increase in the number of patients whose anticoagulation was poorly controlled.[8] In Iran, generic warfarin is mainly supplied by Orion Corporation (Orion Pharmaceutica, Espoo, Finland). The process of import and distribution of this product, for various reasons, is not constant and reliable, imposing serious risks due to unwanted drug discontinuation or dose change. Therefore, we designed this study to compare the efficacy and side-effects of Orion warfarin with two other brands, in order to devise recommendations for the replacement of Orion warfarin with other products when necessary. MATERIAL AND METHODS This was a randomized double-blind crossover clinical trial. The patients were those visiting Modarres Hospital heart clinic, or those hospitalized in Modarres Hospital, who had indications for anticoagulation therapy. All patients had optimal International Normalized Ratio (INR), i.e. 2-3 for atrial fibrillation and 2.5-3.5 for valvular heart disease. Patients were excluded if they did not receive warfarin, could not come to the hospital for weekly visits or did not cooperate, or had diseases interfering with warfarin metabolism. Also, patients on drugs interacting with warfarin such as phenytoin, phenobarbital, cimetidine and amiodarone were excluded. An appropriate review committee approved the study protocol. Patients were briefed on the study protocol and objectives and then, were asked to sign an informed consent if they were willing to participate. The sample size was calculated based on mean necessary dose change in groups assuming alpha=0.05, beta=0.2, SD=0.7 and a difference of 0.5. So 36 patients were randomly allocated into one of the three treatment groups. Each group received one of the study drugs: A (Orion warfarin 5 mg tablets, Orion Pharmaceutica, Espoo, Finland), B (Warf5, CIPLA, Mumbai, India) and C (Warfarin 5 mg tablets, Ferrer, Spain). The formulations were identical in shape and size. The patients and the attending physicians were not aware of the treatments. Each group received the prescribed drug for four weeks. During this period, they were visited weekly. In these weekly visits, prothrombin (PT) and INR were checked and the patients were asked about the possible complications. The attending cardiologist recorded the data and decided whether a dose adjustment was necessary. Target INR was defined according to the indication: 2-3 for atrial fibrillation or 2.5-3.5 for valvular heart disease and prosthetic valves. After four weeks the patients were switched to the next drug (e.g. A to B) and the same method was used. The patients were once more switched to the next drug, till all completed the 12-week duration and had used all the three brands in the course. Blood samples were centrifuged for 5 min and after plasma separation at 37° C, 0.2 ml thromboplastin and 0.1 ml plasma were added to measure PT. Biomerieux table was used to determine INR. Data are presented as percentage and mean+SD. Repeated measures ANOVA was used to assess the differences among the three brands used. A P value less than 0.05 was considered significant. RESULTS The mean age of patients was 51.8±12.7 years. Their average weight was 64.4±14.0 kg. Twenty-four patients were female. Patients received warfarin for the following diagnoses: Valvular heart disease (44.4%), atrial fibrillation (50%), and other conditions (5.6%). The mean number of dose changes throughout the 4-week courses was 1.6±1.2 times for brand A, 1.2±1.1 times for brand B and 1.3±0.9 times for brand C (P=0.24). The amount of total dose changes was similar (0.70±0.6 mg for brand A, 0.63±0.9 mg for brand B and 0.72±0.8 mg for brand C, P=0.89). [Table - 1] shows the amount of dose change in each visit and the total dose change for each brand. [Figure - 1] compares mean INR values in each week for the three brands. Except a sharp and statistically significant increase in INR at the second visit for brand A, the differences between mean INR for the brands in each visit were insignificant. Target INR was defined for each patient according to his/her disease. Patients receiving the three brands achieved the target INR at the same rate (46.9% for brand A, 50% for brand B and 50% for brand C). Thirty-four per cent of patients treated with brand A, 28% of patients treated with brand B, and 32% of patients treated with brand C did not achieve target INR. Over-treatment, i.e. INR>upper limit of target range, was seen in 19%, 22% and 18% of patients treated with brand A, brand B and brand C respectively (P=0.98). The required dose for the stable target INR was 4.6±2.2 mg, 5.3±2.2 mg and 5.3±2.4 mg in patients treated with brand A, B and C respectively (P=0.61). There were no complications except 2 cases of drug discontinuation by the physician for extreme overdose. No major hemorrhagic or thromboembolic events were reported. DISCUSSION The results of this study demonstrated similar effects of the three brands of equal strength (5 mg) oral warfarin (Orion, Cipla and Ferrer). This similarity was demonstrated through the rate of achievement of target INR and number and amount of dose changes. Other studies have examined the effect of switching from one type of warfarin to another. Such studies focus mainly the switch from coumadin to generic warfarin. Most of them have also shown that such a switch is usually harmless and does not have serious effects on anticoagulation. In two randomized crossover clinical trials Neutel and Smith[5] and Handler et al [6] compared coumadin and generic warfarin. They treated patients for 21-28 days. In these trials, the change in the mean baseline INR to overall INR was - 0.10 and -0.20 for Barr and - 0.01 and - 0.02 for DuPont products respectively. Both studies found no significant difference in the average INR values. There was no difference in the adverse effects between the two drugs. Both concluded that the two products were equivalent. Swenson[7] studied a cohort of patients at a managed-care organization and determined the safety and effectiveness of switching to generic warfarin. This study was not blinded and patients seen during routine visits at two anticoagulation clinics were asked to volunteer to use generic warfarin (Barr Laboratories) instead of coumadin for eight weeks. Patients (n = 210) who had therapeutic INR values at the baseline visit and had received anticoagulation with coumadin for three months were enrolled in the study. The control group (n = 105) consisted of patients who declined or were not asked to change the drug. Mean INR values were compared before and after enrollment. The difference between the two groups was not significant and of negligible clinical meaning. Among the patients who had a dosage change, there was no significant difference in the variability of the INR before versus after enrollment. Patients in either group did not report any serious complications. The authors concluded that the two warfarin sodium products were equivalent in usual clinical practice. In one study, Weibert and associates[9] compared the dosing requirements and INRs associated with two bioequivalent crystalline warfarin sodium products in patients with chronic atrial fibrillation. This was a multicenteric, single-blind (prescriber), randomized, crossover trial of Apothecon warfarin and DuPont warfarin (coumadin) in adults with chronic or paroxysmal atrial fibrillation who had been receiving DuPont warfarin chronically for the prevention of thromboembolism. Patients were randomly assigned to initially either continue DuPont warfarin or receive Apothecon warfarin for four weeks, with weekly evaluation of dosage and INR changes, safety and efficacy. Subsequently, patients crossed over and received the other product for four weeks. Neither the propensity for a dosage change or an INR change nor the magnitude of a dosage change or INR change appeared related to a particular warfarin product (NS for each variable after each study period). After four weeks of treatment, the same number of patients (n=7) experienced a 20% change in warfarin dosage from the respective baseline with each product. The number of patients with INRs outside the desired protocol range after four weeks of treatment was similar for both groups (<1.8, n = 9 for both products, or >3.2, n = 9 for DuPont, n=10 for Apothecon). No major hemorrhagic or thromboembolic events occurred. In another cohort study, Milligan and associates[10] determined whether a Health Maintenance Organization (HMO) can add generic warfarin to its formulary without adversely affecting warfarin management or increasing adverse events. Data were collected 8 months prior to and 10 months after the introduction of generic warfarin (Barr Laboratories, Pomona, NY) to an HMO′s formulary. In this study the change did not significantly affect INR control, warfarin management, or adverse events. Authors suggested that HMOs can safely substitute at least 1 generic formulation of warfarin without extra monitoring. In two cases at a family medicine center anticoagulation clinic in Oklahoma city, Hope and Havrda[11] reported sub-therapeutic INR values after a switch from Coumadin to generic warfarin, while all other variables were kept consistent demonstrating the need for close monitoring of the INR when patients are switched between brands of warfarin. Although some findings such as Hope and Havrda′s report[11] underscore the importance of close monitoring if a switch in warfarin brand is done, most studies show safe switch from one warfarin brand to another. This is especially important for our patients, since Orion warfarin is not always available. Since it is very important to maintain a steady and acceptable level of anticoagulation over the time for all the patients, it is sometimes necessary to switch to a different brand when the current brand is not available. Our results demonstrate that such switching is harmless in patients taking warfarin as a prophylactic treatment. REFERENCES
Copyright 2004 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph04128f1.jpg] [ph04128t1.jpg] |
| |||||||||

{kind=link}
{kind=link}