 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
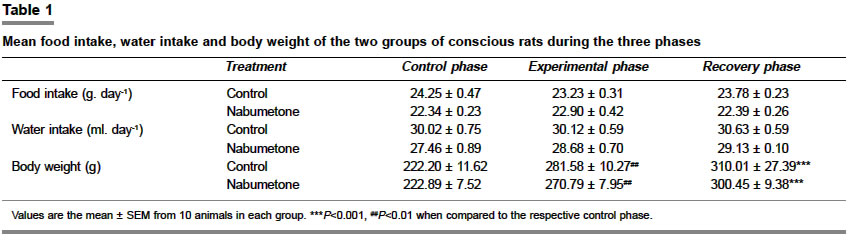
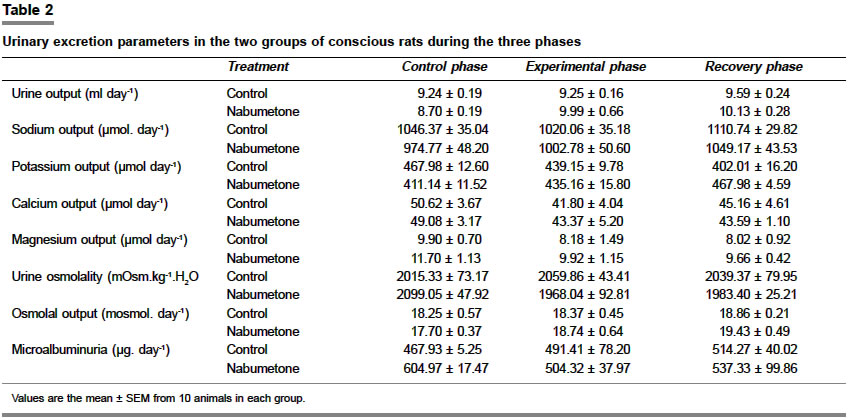
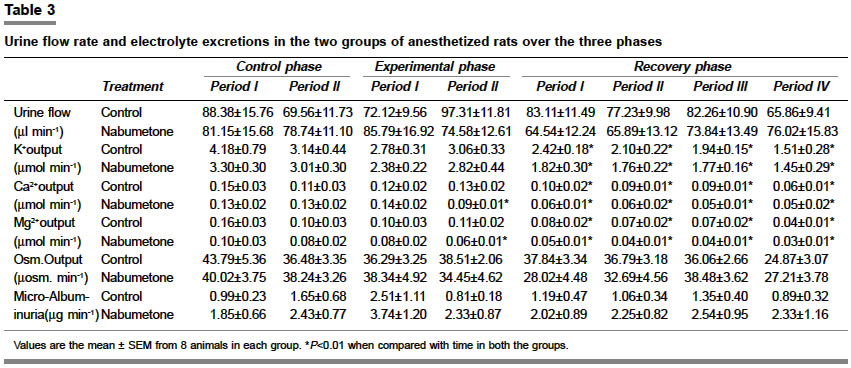
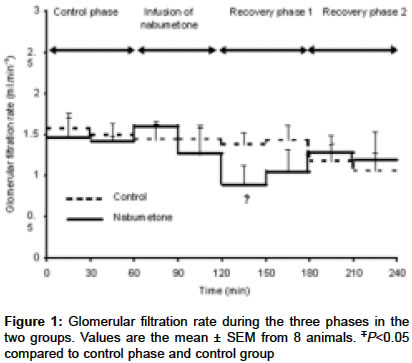
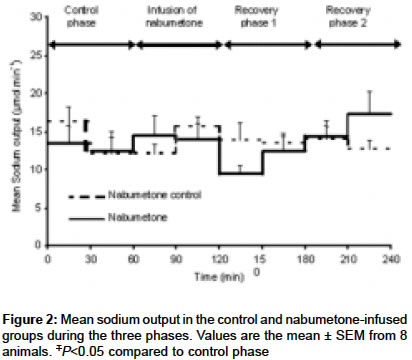
Indian Journal of Pharmacology, Vol. 36, No. 6, November-December, 2004, pp. 363-368 Research Paper Effect of nabumetone on the renal function in conscious and anesthetized rats Long I, Rao GJ, Singh HJ Department of Physiology, School of Medical Sciences, Health Campus, Universiti Sains Malaysia, 16150, Kubang Kerian, Kelantan Code Number: ph04129 ABSTRACT OBJECTIVE: To examine the effect of nabumetone on the renal function in conscious and anesthetized rats.MATERIAL AND METHODS: For the conscious study, rats were housed individually in metabolic chambers for a duration which consisted of acclimatization, control, experimental and a recovery phase comprising 1, 1, 2 and 1 week respectively. During the experimental phase, one group of rats received nabumetone orally and the controls received an equivalent volume of saline. Water and food intake, body weight, urine output, urine osmolality, osmolal output and electrolyte excretions were estimated. In the second study, rats were anesthetized and saline diuresis in these animals was established with an intravenous infusion of 0.9% saline containing 3H-Inulin. Glomerular filtration rate (GFR) was estimated using standard inulin clearance. The study period consisted of equilibration, control, experimental and a recovery phase comprising 2, 1, 1, and 1 hour respectively. During the experimental phase, one group of rats received a bolus dose of nabumetone intravenously and the controls received the vehicle. Blood and urine samples were collected for analysis of electrolytes, microalbuminuria and GFR estimation. Data was analyzed using ANOVA for repeated measurements. RESULTS: In conscious rats, no significant differences were found between the two groups in any of the measured parameters. In anesthetized rats, however, there was a significant but reversible decrease in GFR and sodium excretion in rats receiving nabumetone. CONCLUSION: In contrast to the suggested renal-sparing effects of COX-2 inhibitors, we have observed renal function being affected with nabumetone during anesthetic stress. KEY WORDS: Anesthetic stress, COX-2 inhibitors, kidney function INTRODUCTION Non-steroidal antiinflammatory drugs (NSAIDs) produce deleterious side-effects on renal function, particularly when there is pre-existing renal disease or during hemodynamically stressful situations.[1] These effects have been attributed to the inhibition of prostaglandin synthesis in the kidney by these drugs.[2] When blood volume is compromised or renal blood flow is reduced, prostaglandins play a role in the regulation of renal circulation, renin secretion, and sodium and water excretion.[3] If vasoconstrictive forces stimulated to maintain the filtration fraction during hemodynamically-compromised situations are not balanced by prostaglandin-induced vasodilatation, renal failure may occur. Cyclooxygenase (COX) is a key enzyme regulating the formation of prostaglandins from arachidonic acid. Several years ago, it was reported to have two isoforms, namely, COX-1, the constitutive isoform whose existence was long recognized and COX-2,[4],[5] the inducible isoform. COX-1 is believed to be involved in the production of prostaglandins that help maintain renal function. COX-2, on the other hand, is primarily thought to be involved in the production of prostaglandins during inflammatory processes.[6] These assumptions formed the basis of the "COX hypothesis" which proposes that COX-1-derived prostaglandins are involved in regulating physiological functions, whereas COX-2 derived prostaglandins play a major role during inflammation or tissue damage. Thus, it was assumed that a selective COX-2 inhibition can provide potent therapeutic effects without the side-effects that are observed with the non-selective non-steroidal antiinflammatory drugs (NSAIDs).[7] However, recent reports point to the presence of COX-2 in the macula densa and surrounding cortical cells of the thick ascending limb of the loop of Henle (TALH) of a normal rat,[8] suggesting that it may have a normal physiological role. Furthermore, in the rabbit, COX-2 in TALH epithelial cells in the tubuloglomerular contact region play an important role in the control of renin secretion by macula densa.[9] In fact, COX-2 mRNA and protein expression in the mammalian kidney are among the highest observed in any tissues.[10] COX-1, on the other hand, has been shown to be involved in inflammatory reactions.[11] These observations suggest that COX-1 and COX-2 may not have such clearly demarcated roles as proposed by the "COX-hypothesis" and renal deleterious effects may still be observed with selective COX-2 inhibitors. We therefore examined the effect of nabumetone, a selective COX-2 inhibitor, on renal function in conscious and anesthetized rats. MATERIAL AND METHODS For experiments on conscious rats, male Sprague-Dawley rats weighing between 200-220 g were housed individually in metabolic cages for a total duration of 5 weeks. The animal unit of Health Campus, Universiti Sains Malaysia supplied the rats used in this study. The study protocol consisted of four phases, namely, acclimatization phase (1 week), control phase (1 week), experimental phase (2 weeks) and recovery phase (1 week). All animals were treated identically during the acclimatization, control and the recovery phases. No observations were made during the acclimatization phase where the animals were allowed to acquaint themselves with the metabolic cages. During the experimental phase, however, the animals in the nabumetone group (n=10) were given 15 mg/kg/day of nabumetone dissolved in 0.5 ml of saline via the oral route. The dose that was administered is equivalent to the maximum therapeutic dose used in humans. Animals in the control group (n=10) received only 0.5 ml of saline orally. Food and water intake, body weight, urine output, urine osmolality, urinary osmolal output, urinary excretions of sodium, potassium, magnesium, calcium and microalbumin were estimated in all animals over 24 h on alternate days during the control, experimental and recovery phases. For experiments on anesthetized animals, male Sprague-Dawley rats weighing between 230-260 g, fasted overnight but with access to water ad libitum, were prepared for standard inulin clearance experiments.[12] Following anesthetization with an intraperitoneal injection of sodium thiopental (60 mg/kg, body weight), the jugular vein and carotid artery were cannulated for continuous normal saline infusion, and blood pressure monitoring and blood sampling respectively. Tracheostomy was performed to maintain a clear airway. The urinary bladder was catheterized suprapubically for urine collection. Animals were infused intravenously with 0.9% saline, containing 3H Inulin (0.5 µCi ml-1, Amersham, UK), at a rate of 200 µl min-1 for the first hour to induce rapid volume expansion and diuresis. The infusion rate was then reduced to 100 µl min-1 of 0.9% saline containing 3H Inulin (1 µCi ml-1) for the next five hours. The five hours were divided into four phases, namely equilibration phase (1 h), control phase (1 h) experimental phase (1 h), and recovery phase (2 h). There were two groups of rats, the experimental group (n=8), which consisted of animals receiving nabumetone intravenously (5 mg/kg body weight) at a rate of 100 µl min-1 during the experimental phase (one hour), and the control group (n=8), which consisted of animals receiving the vehicle (0.1 ml acetone) during the same period. Blood and urine samples were collected every 30 min for analyses of urinary osmolality, urinary osmolal output, urinary microalbumin and glomerular filtration rate (GFR) estimation. Urinary sodium and potassium concentrations were analyzed using a flame photometer (Corning 404, UK), urinary magnesium and calcium concentrations were analyzed using ion selective electrodes (Hitachi-912), urinary osmolality was estimated by the freezing point depression (Osmomat 030, Gonotec, Germany) and urinary microalbumin was estimated using a commercially available kit for human urinary microalbumin (SERA-PAK, Bayer, USA). Statistical analysis was performed using two-way ANOVA for repeated measurements and Tukey Post Hoc for multiple comparisons to locate the differences when ANOVA revealed a significant effect. All results were presented as mean ± SEM and a P′ Value of 0.05 or less considered as significant. The Universiti Sains Malaysia Ethics Committee approved the study protocol. RESULTS Food intake, water intake and body weight were measured every two days. As there were no significant differences between the values in each rat in each phase, the values for each phase for each rat were averaged and the average was then used to calculate the group mean. No significant differences were evident in food and water intake when the three phases in each group were compared or when the corresponding phases of the two groups were compared ([Table - 1]). Body weight increased significantly in both the groups over the period of the study, but no significant differences were evident in the rate of increase in body weight between the two groups. Urinary parameters (urine output, sodium output, potassium output, calcium output, magnesium output, urine osmolality, osmolal output and microalbuminuria) were measured every two days. As there were no significant changes over time between the values during each phase, the values for each rat in each phase were averaged and the average was then used to calculate the group mean ([Table - 2]). No statistically significant differences were evident in any of the measured urinary parameters between the three phases in each group or between the corresponding phases of the two groups. In anesthetized rats, no significant differences were observed in the urine flow rate, osmolal output and microalbuminuria over the duration of the study in both the groups or between the two groups when the corresponding periods in the three phases were compared ([Table - 3]). Calcium, magnesium and potassium excretions were found to decrease significantly with time in both the groups (P<0.01). However, when the corresponding periods in the three phases of the two groups were compared for these parameters, there were no significant differences between the excretion rates of these electrolytes. All values in the table have been rounded up to two decimal places. No significant difference was evident in the mean GFR between the two groups during the control phase ([Figure - 1]). Mean GFR remained stable throughout the period of study in the control rats, except during the final recovery period where it declined slightly, but non-significantly, when compared to that during the control phase. About 30 min after the commencement of nabumetone infusion, GFR began to decline and it continued to decline during the first half hour of the recovery phase where mean GFR was significantly lower than that during the control phase and also significantly lower than that in the corresponding period of the control rats (P<0.05). GFR began to recover over the second collection period of the recovery phase reaching values similar to those in the control animals by the final period of the recovery phase. No significant difference was evident in the mean urinary sodium excretion between the two groups during the control phase ([Figure - 2]). Mean sodium excretion remained stable throughout the three phases in the control rats. Nabumetone infusion resulted in a significant decline in the mean urinary sodium excretion during the first 30 min of the recovery phase 1 (P<0.05). After that the mean sodium excretion in the nabumetone-infused rats increased and reached the levels of that of control rats during the final three recovery periods. DISCUSSION Most of the renal studies investigating the effects of NSAIDs on animals were done on animals that had been anesthetized and had surgery performed on them. Anesthesia and surgery depress renal function in the rat.[12],[13] Both anesthetization and surgery place considerable stress on the animal, and this possibly itself induces increased renal prostaglandin synthesis. Results from anesthetized rats, therefore, cannot always be extrapolated to conscious rats. We therefore investigated the effect of nabumetone on conscious and anesthetized rats to see if the effects of nabumetone were similar or different in these two states. We were unable to measure GFR in the conscious animals and our assessment of renal function in these animals is therefore based on the seven urinary parameters that were measured ([Table - 2]). We had earlier used a similar protocol to demonstrate the effects of naproxen on the renal function in conscious rats where we found evidence of a reversible increase in urine output and microalbuminuria.[14] Administration of nabumetone at a dose of 15 mg/kg body weight, for a period of two weeks, appears not to have affected the measured renal parameters, when compared to those in age-matched controls ([Table - 2]). In addition, no significant differences were evident in food and water intake or body weight between the two groups ([Table - 1]). The absence of any obvious renal effects following nabumetone administration is not surprising as under euvolaemic conditions, renal prostaglandin synthesis is low and it is therefore not possible to demonstrate an important role for prostaglandins in maintaining renal function. Our findings further confirm this. In situations where the systemic circulation is destabilized or compromised, prostaglandins exert a compensating influence on renal function. Numerous studies have identified patients with decreased effective arterial blood volume,[15] e.g. those with hypertension, congestive heart failure and diabetic nephropathy[16] and the aged,[17] as being at risk for renal complications when given NSAIDs. This is because in these disease states there is possibly an increased dependence on prostaglandins for the maintenance of renal function.[18] All the animals in this study were healthy and normal. The absence of any significant difference in renal function from the controls following the administration of nabumetone at a dose of 15 mg/kg body weight, also suggests that COX-2 may not have an important role in renal fluid and electrolyte homeostasis under normal circumstances. It has however to be added that the dose used was not the maximum dose for a rat but the maximum therapeutic dose used in humans and it was given once a day, in view of its long half-life. We do not know if higher doses would have given similar or different results. In the anesthetized animals, urine output, GFR and excretion rates of all the electrolytes during the control period were similar in both the groups ([Table - 3], [Figure - 1] and [Figure - 2] and were within the range reported in the literature using similar protocols.[19] Although the infusion rate was 100 mlmin-1, urine output averaged between 75-85 mlmin-1in all the rats. This inability of the anesthetized animal to excrete completely the infused saline load has been reported before and the reason for this is not clearly established.[19] Administration of nabumetone intravenously to anesthetized rats significantly decreased GFR and sodium excretion, albeit transiently [Figure - 1] and [Figure - 2]. Both GFR and sodium excretion decreased immediately after the infusion of nabumetone. During the first half hour of the recovery phase, GFR and sodium excretion were significantly lower (P<0.05) than that in the corresponding periods of the control animals. Interestingly, no significant differences were evident in the excretions of calcium, magnesium, potassium or microalbuminuria between the corresponding phases of the two groups. Excretion rates of calcium, magnesium and potassium decreased with time and the decreases were similar in both the groups. This may be due to their increased tubular reabsorption secondary to the activation of mechanisms that help maintain their homeostasis, as none of these electrolytes was present in the infusates. Such excretion patterns however, have been reported before.[19] Effects of selective COX-2 inhibitors on renal function have been reported in the dog,[20] and the rat,[21] although in the latter study, impaired renal function was only evident in isolated perfused kidneys of rats pretreated with oral nabumetone but not in kidneys when left in vivo. The reason for this discrepancy is unclear but it may reflect the severity of the procedures involved and possibly the role of some extra-renal mechanisms in the maintenance of renal function. The precise mechanism responsible for the fall in GFR following nabumetone infusion is unclear. The stress of anesthesia and surgery increases renal sympathetic activity and causes vasoconstriction in the kidney, thereby decreasing renal blood flow and consequently GFR. Normally, in the absence of COX inhibitors, prostaglandin-induced vasodilatation would have opposed the vasoconstrictor effects of the renal sympathetic nervous system[4] and attenuated the vasoconstrictor responses to norepinephrine.[3] Recent evidence suggests that noradrenalin enhances the production of COX-2 derived metabolites, which then play an important role in modulating the renal vasoconstriction elicited by noradrenaline.[22] In the presence of nabumetone, this balance between the vasoconstrictor and vasodilators forces could have been disturbed and GFR decreased. The fall in sodium excretion was even more significant given the fact that approximately 150 mmol min-1 was continuously infused throughout the period of study. Two possible mechanisms could also explain the decreased sodium excretion evident with nabumetone infusion. The first is associated with decreased GFR, where a decrease in GFR would result in decreased filtered load and consequently a decrease in urinary excretion of sodium. The second mechanism may be due to the removal of the inhibitory effect of prostaglandins on tubular sodium reabsorption. Prostaglandins are both diuretic and natriuretic in their action.[23] They have been shown in vitro to directly inhibit tubular reabsorption of sodium[24] and water.[25] The decrease or absence of prostaglandins in the presence of nabumetone, may increase tubular reabsorption of sodium and consequently decrease its excretion in the urine. There may well be other mechanism/s that are involved in these responses, as prostaglandins also influence the regulation of medullary blood flow, which contributes to the kidney′s ability to modify renal solute excretion. Clearly, further studies using different doses of these drugs are needed to elucidate the responses of the kidneys to different COX inhibitors in different situations. In addition, this makes a good point for further investigations into the expression of the isoenzyme in the rat nephron in normal and during stressful situations. In conclusion, our study suggests that firstly, COX-2 derived prostaglandins are possibly not involved in the maintenance of renal function in the rat in normal situations. This, however, would require further confirmation with higher doses. Secondly, COX-2 derived prostaglandins are involved in the maintenance of GFR and sodium excretion, particularly in anesthetized rats. It may therefore be added that in hemodynamically stressful situations, selective COX-2 inhibitors can have similar renal effects as non-selective NSAIDs. ACKNOWLEDGEMENTS This research study was supported by a short-term grant from Universiti Sains Malaysia. REFERENCES
Copyright 2004 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph04129f2.jpg] [ph04129t3.jpg] [ph04129t2.jpg] [ph04129t1.jpg] [ph04129f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}