 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
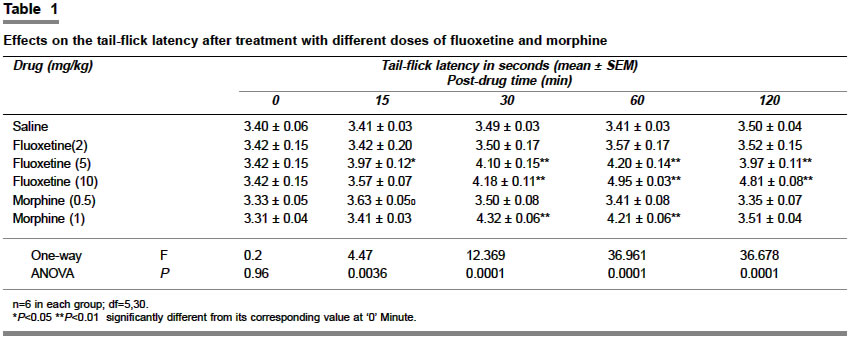
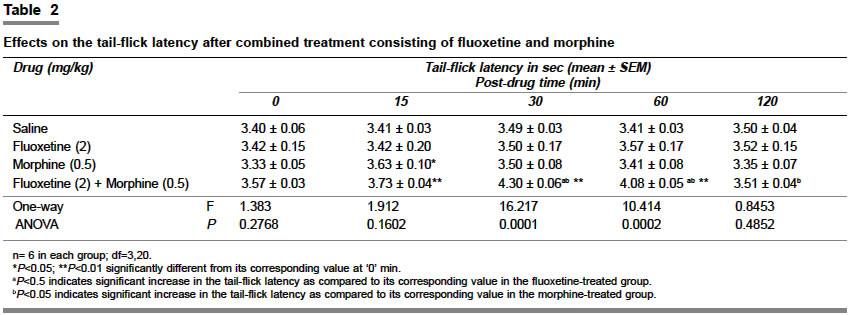
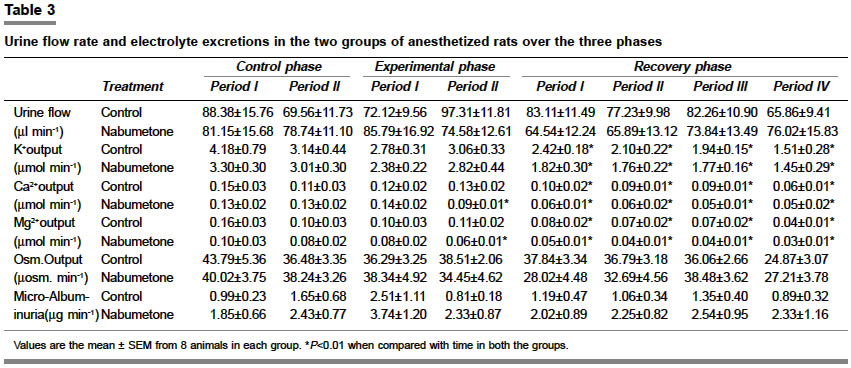
Indian Journal of Pharmacology, Vol. 36, No. 6, November-December, 2004, pp. 369-372 Research Paper Study of the antinociceptive activity of fluoxetine and its interaction with morphine and naloxone in mice Kurlekar PN, Bhatt JagatD Department of Pharmacology, Medical College, Baroda - 390 001 Code Number: ph04131 ABSTRACT OBJECTIVE: To study the probable site of the antinociceptive action of fluoxetine and its interaction with morphine and naloxone.MATERIAL AND METHODS: The antinociceptive activity of fluoxetine was studied using tail-flick method in the absence and presence of naloxone in mice. Different doses of fluoxetine (2, 5 and 10 mg/kg) and morphine (0.5 mg/kg and 1 mg/kg) were administered subcutaneously to select the subanalgesic doses for both. Subanalgesic doses of both the drugs were administered simultaneously to study their interaction on tail-flick latency. RESULTS: Fluoxetine and morphine produced a dose-dependent antinociceptive action. Combination of the subanalgesic dose of both fluoxetine (2 mg/kg) and morphine (0.5 mg/kg) produced an additive effect. Naloxone in a dose of 1 mg/kg produced a significant (P<0. 001) hyperalgesia at time intervals of 15, 30 and 60 min while in a dose of 2 mg/kg it produced significant (P<0. 001) hyperalgesia at time intervals of 30, 60 and 120 min. Naloxone (2 mg/kg) pretreatment significantly reduced the antinociception produced by fluoxetine. CONCLUSION: Analgesia produced by fluoxetine may be mediated by 'µ' opioid receptor, however, mechanisms involving other endogenous opioid peptides could not be ruled out. Fluoxetine as a monotherapy or in combination with other opioids could be useful in the management of pain. KEY WORDS: Analgesia, SSRI, opioids INTRODUCTION Pain is an unpleasant sensation, and a very common phenomenon. There is no doubt that pain acts as a warning signal against disturbances either in the body or in the external environment of an individual. The principal objective of the treatment of pain is to remove or abolish the cause of pain. But it is not always possible to do so; hence, analgesics are used for the symptomatic treatment of pain. Opioids are the most potent and commonly used group of analgesic drugs e.g. morphine and pethidine. But their analgesic action is associated with a greater degree of adverse drug reactions, most of which are dose-dependent. Recently, numerous open and controlled studies have shown that antidepressant drugs also have analgesic activity and particularly, selective serotonin reuptake inhibitors (SSRI) are effective in mixed, chronic pain.[1] It has also been shown that some antidepressants are superior to placebo in about 75% of studies.[2] A wide range of pain conditions are responsive to antidepressants, particularly diabetic neuropathy pain and probably rheumatoid arthritis,[3] and migraine.[4] SSRIs inhibit the reuptake of the serotonin (5-HT), increase the level of 5-HT in the neuronal synapse, and facilitate serotonergic activity. This mechanism may be involved in the antinociceptive effect of antidepressants.[5] However, the exact mechanism of its analgesic activity remains to be fully understood. Therefore the present study was planned to (1) demonstrate the analgesic activity of fluoxetine and (2) to study the interaction of fluoxetine with morphine and to delineate the probable site of action of fluoxetine in the experimental model of acute pain using mice. MATERIAL AND METHODS Albino mice of either sex (25-35 g), maintained at an ambient temperature of 25-35° C with food and water ad libitum were used. The animals were divided into groups of six each. Group I: Received vehicle (saline); Groups II, III and IV received fluoxetine (2, 5 and 10 mg/kg); Groups V and VI received morphine (0.5 mg/kg and 1 mg/kg); Group VII received combined treatment consisting of fluoxetine (2 mg/kg) and morphine (0.5 mg/kg); Group VIII received combined treatment consisting of fluoxetine (5 mg/kg) and naloxone (1 mg/kg). Group IX received combined treatment consisting of fluoxetine (5 mg/kg) and naloxone (2mg/kg); Groups X and XI received naloxone (1 mg/kg and 2 mg/kg). In the groups which received combined treatment, both the drugs were administered simultaneously at different sites. All the drugs were administered subcutaneously. Schedules of drugs administration In all the groups the antinociceptive test was performed at time intervals of 0, 15, 30, 60 and 120 min after the administration of drugs or the vehicle. However, naloxone was administered 10 min prior to the administration of fluoxetine. Determination of antinociceptive activity Antinociceptive activity was measured by the tail flick method[6] using analgesiometer. The animals were exposed to noxious stimulus (i.e. radiant heat) and tail flick latencies (the time required for the flicking of tail i.e. the reaction time) and a mean of two pre-drug recordings were taken as basal value (0 min). In order to prevent tissue injury a cut-off time of 10 seconds (based on the reaction time, which generally varied between 3-4 sec) was maintained. In animals not responding up to 10 sec, the cut-off time was considered as the latency.[7] Drugs and chemicals A stock solution of fluoxetine (Sigma St.Louis), morphine (British Medicine Pharmaceuticals Company), and naloxone (Dupont) were prepared freshly on the day of the experiment in isotonic saline (0.9% NaCl) and administered in total volume of 0.1 ml. Statistical analysis The results are expressed as mean±SEM, unpaired Student′s ′ t ′ test was employed for comparison between the two means as a measure of significance. One-way ANOVA was applied for comparison amongst different groups. P Value of <0.05 was regarded as a statistically significant value. RESULTS Effects of saline treatment: In the saline-treated animals there were no significant changes in the tail-flick latency during the entire test period of 120 min ([Table - 1]). Effects of fluoxetine treatment: Fluoxetine at a dose of 2 mg/kg showed no significant effect on the tail-flick latency as compared to the corresponding 0 minute values ([Table - 1]). Fluoxetine in a dose of 5 mg/kg produced a significant increase in the tail-flick latency at all time intervals with onset of antinociceptive effect at 15 min (P<0.05) and maximum effect at 60 min (P<0.01). At a dose of 10 mg/kg fluoxetine showed significant (P<0.01 to P<0.001) antinociceptive effect at intervals of 30, 60 and 120 min ([Table - 1]). Thus fluoxetine produced a dose-dependent antinociception. Effects of morphine treatment: Morphine at a dose of 0.5 mg/kg produced a significant increase in tail-flick latency after 15 min as compared to its corresponding value at 0 min; with no significant change in latency over the remaining period ([Table - 1]). However, at a dose of 1 mg/kg, morphine produced a significant increase in tail-flick latency at 15 min that persisted during the entire test period of 120 min. The peak effect was seen at 30 min ([Table - 1]). Thus morphine produced dose-dependent increase in the tail-flick latency. Effects of combined treatment with fluoxetine and morphine Since fluoxetine and morphine at 2 mg/kg and 0.5 mg/kg respectively did not produce any significant change in tail-flick latency they were considered as subanalgesic doses. The combination of subanalgesic doses of fluoxetine (2 mg/kg) and morphine (0.5 mg/kg) produced a significant (P<0.01 to P< 0. 001) increase in the tail-flick latency at 15 min, which lasted up to 60 min with a peak response at 30 min ([Table - 2]). Effects of naloxone treatment Naloxone at a dose of 1 mg/kg produced a significant (P<0.01 to P<0.001) decrease in the tail-flick latency (hyperalgesia) at intervals of 15, 30 and 60 minutes while at 2 mg/kg it lasted even at 120 min ([Table - 3]). Effects of combined treatment with fluoxetine and naloxone In animals who received combined treatment of naloxone (1 mg/kg) and fluoxetine (5 mg/kg) there was significant (P<0.01 to P<0.001) increase in tail-flick latency. However, with a higher dose of naloxone (2 mg/kg) and fluoxetine (5 mg/kg) there was no significant change in the tail-flick latency during the entire test period ([Table - 3]). Thus pre-treatment with naloxone at a dose of 2 mg/kg completely antagonized the antinociceptive effect of fluoxetine (5 mg/kg). DISCUSSION Pain is an unpleasant sensory or emotional experience associated with actual or potential tissue damage. Pain is always a subjective feeling. Many people report pain in the absence of tissue damage or any likely pathophysiological cause. One of the objectives of the treatment of pain is to remove the cause of pain. Opioids have been the mainstay of pain treatment for thousands of years and remain so even today. Opioids exert their therapeutic effect by mimicking the action of endogenous opioid peptides at opioid receptors.[8] Several clinical and laboratory studies have reported antinociceptive activity of antidepressants.[9],[10],[11] Antidepressants are reported to be more effective than opioid analgesics in treating neuropathic or deafferentiation pain.[12] Inhibition of the reuptake of monoamines is considered to be a major effect of antidepressants.[13] In the present study, fluoxetine caused a dose-dependent antinociceptive effect. Opioid or opioid-like activity of fluoxetine and some other SSRIs has been reported in some binding assays.[14],[15] Some studies have disputed the affinity of fluoxetine for opioid receptors.[11],[16] It is not clear whether or not opioid receptors are involved in the analgesic activity of fluoxetine and if so to what extent. The actions of morphine are mainly antagonized by opioid antagonist naloxone. Naloxone produces very little effect in normal subjects, but produces rapid reversal of the effect of morphine and also the partial agonists such as pentazocine and nalorphine.[17] It has little effect on the pain threshold under conditions of stress or inflammation when endogenous peptides are produced.[15] Recently, Rafiran-Kopaei and Swell[2] and Singh et al [4] reported that fluoxetine-induced antinociception was antagonized by naloxone. Also, fluoxetine did not exhibit any antinociceptive effect in serotonin-depleted animals.[4] Our findings are in agreement with the above observation. Thus it likely that fluoxetine acts through opioid pathways involving the µ opioid receptor. However, most antidepressants interact with other receptor systems, which have been characterized as cholinergic, muscaranic, histaminic, noradregenic and even GABAergic system.[13],[18] In all instances some pathways carrying these receptors are able to elicit analgesic activity.[19],[20] So it would not be unreasonable to suggest that antidepressant drugs would involve at least some of these systems in the mediation of their analgesic effect. Fluoxetine has been reported to be useful clinically in some cases such as diabetic neuropathy and migraine.[4] It has been suggested that the antinociceptive activity of antidepressants might be due to their antidepressant action. However, the antinociceptive action of fluoxetine was observed much earlier and even with a lower dose than that required to achieve antidepressant effects. Therefore it is likely that opioid or opioid-like activity may be playing an important role in fluoxetine-induced antinociceptive action. An enhancement of opioid-induced antinociception by antidepressants has been demonstrated.[11],[20] Similarly, in the present study, a combination of the subanalgesic doses of morphine and fluoxetine produced a significant increase in the tail-flick latency suggesting additive antinociceptive action. Therefore the above combination therapy would theoretically minimize the dose requirements and thus the potential adverse effects, though clinical studies are needed to prove the same. REFERENCES
Copyright 2004 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph04131t1.jpg] [ph04131t3.jpg] [ph04131t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}