 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 36, No. 6, November-December, 2004, pp. 373-376 Research Paper Effect of shilajit on blood glucose and lipid profile in alloxan-induced diabetic rats Trivedi NA, Mazumdar B, Bhatt JD, Hemavathi KG Department of Pharmacology, Medical College, Baroda - 390 001 Code Number: ph04132 ABSTRACT OBJECTIVE: To study the effect of shilajit (a herbomineral preparation) on blood glucose and lipid profile in euglycemic and alloxan-induced diabetic rats and its effects on the above parameters in combination with conventional antidiabetic drugs.
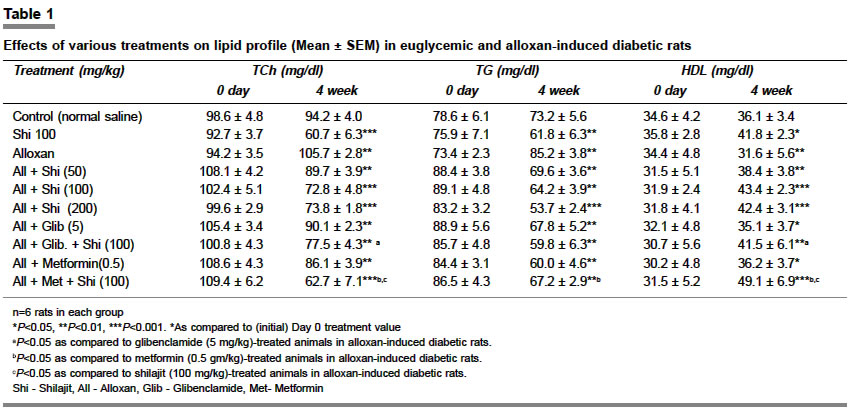
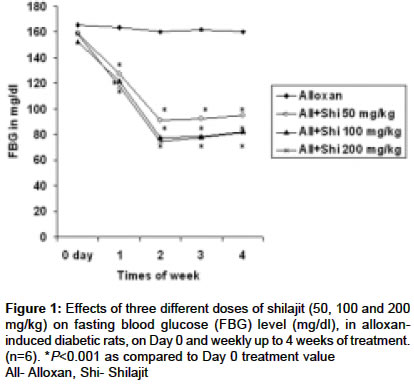
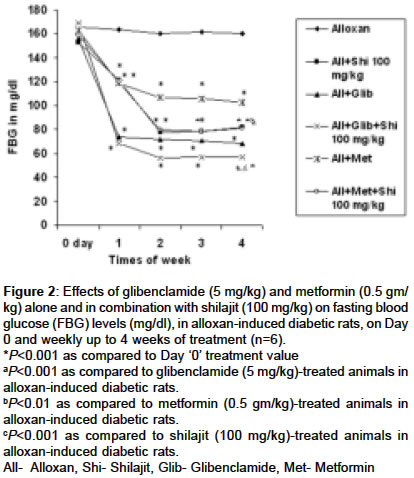
KEY WORDS: Biguanide, diabetes mellitus, herbomineral antidiabetic, sulfonylurea. INTRODUCTION Diabetes mellitus is a major public health problem in the developed as well as developing countries. It is ranked seventh among the leading causes of death, and third when all its fatal complications are taken into account. Large-vessel atherosclerosis is the most common cause of death in diabetics. An ideal oral treatment for diabetes would be a drug that not only controls the glycemic level but also prevents the development of atherosclerosis and other complications of diabetes. Unfortunately, among the currently available drugs, the choice is very limited. Alloxan is widely used to induce experimental diabetes and is associated with marked reduction in islet cell Super Oxide Dismutase (SOD) activity.[1] Shilajit is a herbo-mineral drug, which oozes out from a special type of mountain rocks in the peak summer months. It is found at high altitudes ranging from 1000 to 5000 meters. The active constituent of shilajit consists of dibenzo-alpha-pyrones and related metabolites, small peptides (constituting non-protein amino acids), some lipids and carrier molecules (fulvic acids).[2],[3] Standard shilajit contains at least 5-7% dibenzo-alpha-pyrones.[2],[3],[4] Shilajit finds extensive use in Ayurveda, for diverse clinical conditions. For centuries people living in the isolated villages in Himalaya and adjoining regions have used shilajit alone or in combination with other plant remedies to prevent and combat problems with diabetes.[5] Medical researchers have taken a more serious interest in determining if the claims regarding the antidiabetic effects of shilajit have scientific merit. Studies done by Gupta[6] and Bhattacharya[7] have also reported the antidiabetic actions of shilajit. In the light of the above data, the objectives of the present study were to evaluate (1) the effect of shilajit on blood glucose and lipid profile in euglycemic and alloxan-induced diabetic rats and (2) to study its effect on the above parameters in combination with conventional oral antidiabetic agents. MATERIAL AND METHODS Animals Adult albino rats (250-300 gm) of either sex were used for the study. They were housed at ambient temperature of 25±2°C and 45-55% humidity, with 12 h light dark cycle. Animals were fed with standard laboratory diet and water was given ad libitum. Animals described as fasted were deprived of food for 18 h but had free access to water. Study design Each group consisting of six animals received the following treatment. The first group of rats received normal saline (vehicle of alloxan), which served as a euglycemic control, while the second group received shilajit (100 mg/kg, p.o.). A single dose (125 mg/kg, i.p.) of alloxan monohydrate 5% (dissolved in normal saline) was used for induction of diabetes mellitus in the rats. The induction of diabetes mellitus was confirmed after the 5th day of alloxan treatment by estimation of elevated fasting blood glucose (FBG) level. Only those rats with blood glucose level 150 > mg/dl were included in the study (Day 0). These rats were further divided into various groups as follows: Group 3 served as diabetic control. While Groups 4, 5 and 6 were treated with three different doses of shilajit (50, 100 and 200 mg/kg/day/p.o. respectively). Groups 7 and 8 were treated with glibenclamide (5 mg/kg, p.o.) and a combination of glibenclamide (5 mg/kg) with shilajit (100 mg/kg) respectively while Groups 9 and 10 received metformin (0.5 gm/kg, p.o.) and a combination of metformin (0.5 gm/kg) with shilajit (100 mg/kg) respectively. Treatment with drugs was started on the 6th day of the alloxan treatment (i.e. Day 1) and was continued for 4 weeks. All the drugs were given orally as a single dose in the morning. Blood glucose was measured before starting the treatment (Day 0) and weekly thereafter up to the end of the treatment period. Total cholesterol (TCh), triglyceride (TG) and high-density lipoprotein (HDL) (i.e. lipid profile) were measured on Day 0 and after the completion of the treatment period (i.e. at the end of the 4th week). Blood was collected by cardiac puncture just before drug administration and 24 h after completion of the treatment. Blood glucose and lipid profile were estimated by enzymatic method using reagent kit (Span diagnostic Ltd., Surat, India). Statistical analysis The results are expressed as mean±SEM. Data on blood glucose level were analyzed by one-way ANOVA followed by Tukey′s post hoc test. While data on lipid profile were analyzed by Student′s ′t ′ test. Value of P less than 5% (P<0.05) was considered statistically significant. RESULTS A steady decrease in the body weight was observed in the alloxan-treated rats which was significant after the 2nd week of alloxan treatment. Shilajit per se had no effect on body weight but attenuated the weight loss observed in alloxan-induced diabetic rats (data not shown). Effects of shilajit on euglycemic rats A significant (P<0.001) reduction in the blood glucose level was observed at the end of 2nd week of treatment with shilajit (100 mg/kg) in the euglycemic rats, which remained persistent up to 4 weeks of the treatment period (data not shown). Moreover, a significant reduction in the level of TCh (P<0.001) and TG (P<0.01) with significant increase (P<0.05) in the level of HDL was noted at the end of the 4th week of treatment as compared to the Day 0 value [Table - 1]. Effects of shilajit on alloxan-induced diabetic rats In alloxan-treated rats, the rise in blood glucose level reached its peak value on the 5th day and then remained stable throughout the study period [Figure - 1]. Treatment with all the three doses of shilajit (50, 100 and 200 mg/kg) produced significant reduction in the blood glucose level with maximum reduction being achieved with the dose 100 mg/kg (P<0.001). The peak reduction in blood glucose level with all the three doses was observed at the end of the 2nd week of treatment, which remained stable up to the 4th week [Figure - 1]. Similar effects were also observed in the lipid profile. Treatment with 50, 100 and 200 mg/kg of shilajit produced significant reduction in TCh level, with maximum reduction caused by 100 mg/kg (P<0.001). There was dose-dependent reduction in the TG level. All the three doses of shilajit also produced significant increase in the HDL level with the maximum elevation being produced with the dose of 100 mg/kg (P<0.001) [Table - 1]. Effect of shilajit in combination with known antidiabetic drugs Combination of shilajit with glibenclamide significantly (P<0.001) enhanced the glucose-lowering effect of shilajit (100 mg/kg) (P<0.05) or glibenclamide (P<0.01) per se [Figure - 2]. Moreover, the effect of the combination treatment on the lipid profile was significantly more than that of glibenclamide per se (P<0.05), however, it was comparable to that produced by shilajit (100 mg/kg) per se [Table - 1]. Combination of shilajit (100 mg/kg) with metformin significantly lowered the blood glucose level compared to that of metformin per se (P<0.01). However, it was comparable to that of shilajit (100 mg/kg). Moreover, the combination treatment caused significant improvement in the lipid profile as compared to that of shilajit (100 mg/kg) (P<0.05) or metformin (P<0.05) per se. DISCUSSION Although the precise mechanism of alloxan-induced diabetes remains unclear, there is increasing evidence that it involves the degeneration of islet b-cells by accumulation of cytotoxic free radicals.[1] Following its administration, alloxan is concentrated in the islets and in the liver, where it is reduced to dialuric acid. This acid is unstable in aqueous solutions and undergoes oxidation back to alloxan, accompanied by generation of O2-, hydrogen peroxide and hydroxyl radicals by Fenton type reaction.[1] The liver contains high super oxide dismutase (SOD), catalase and glutathione peroxidase activities, which can scavenge these free radicals. On the contrary, the islet cells have low concentrations of these enzymes and are vulnerable to the cytotoxic effects of the free radicals. It is reported that increase in islet cell SOD activity can prevent or decrease alloxan toxicity.[1] Experimental diabetes is suggested to result from initial islet inflammation, followed by infiltration of activated macrophages and lymphocytes in the inflammatory focus. These cells might be the source of the cytotoxic oxygen radicals. Shilajit has been reported to reduce macrophage and lymphocyte activation and migration, as a part of its immunomodulatory activity.[7] Moreover, being an antioxidant it will prevent damage to the pancreatic islet cell induced by the cytotoxic oxygen radicals.[7],[8],[9] In the present study, treatment with shilajit (100 mg/kg) in euglycemic rats produced significant hypoglycemia. Gupta et al[6] suggested that long-term treatment with shilajit increases the number of b-cells of pancreas, i.e. pancreatotrophic action, which may result in better sensitivity of pancreatic b-cells with prompt secretion of a large quantity of insulin in response to hyperglycemia. Combination of shilajit with glibenclamide produced a significant decrease in the blood glucose level which is higher than that produced by either drug alone. Thus it seems likely that, apart from it′s pancreatic action, shilajit may also possess extrapancreatic action, which could have contributed to its hypoglycemic action. The hypoglycemic effect of shilajit (100 mg/kg) is significantly higher than that of metformin (500 mg/kg). But the combination of shilajit with metformin produced no further significant reduction in the blood glucose level compared to that produced by shilajit (100 mg/kg) per se. All the three doses of shilajit also produced a significant beneficial effect on the lipid profile in alloxan-induced diabetic rats. It is reported that the derangement of glucose, fat and protein metabolism during diabetes, results into the development of hyperlipidemia.[10],[11],[12] The beneficial effects on the lipid profile by shilajit in alloxan-induced diabetic rats may be secondary to better glycemic control. Moreover, shilajit produced significant beneficial effects in the lipid profile in euglycemic rats also by reducing TCh and TG and increasing HDL significantly. Therefore, it is likely that shilajit-induced favorable changes in the lipid profile in diabetic rats may not only be due to better glycemic control (secondary), but could also be due to its direct action on lipid metabolic pathways. Combination of glibenclamide with shilajit failed to produce significant improvement in the lipid profile than that produced by shilajit (100 mg/kg) per se. This could be explained on the basis that improvement in the lipid profile by glibenclamide in diabetic rats may be due to better glycemic control (i.e. secondary).[13] Since glibenclamide acts by secondary mechanism, further improvement in the lipid profile was not observed when used with shilajit. The effect on the lipid profile produced by combination treatment is significantly (P< 0.01) more than that produced by glibenclamide per se. Metformin produces beneficial effects on the lipid profile mainly by correcting abnormal glucose metabolism.[14] It also produces moderate reduction in the triglyceride levels as a result of decreased hepatic synthesis of very low-density lipoprotein.[13] A similar observation has been reported in our study. Metformin has also been found to reduce the postprandial hyperlipoproteinemia of intestinal origin significantly.[13] Since the combination of shilajit with metformin produced further improvement in the lipid profile except TG, than that produced by metformin or Shilajit per se, it is suggested that shilajit may be acting by some different mechanism than that of metformin on lipid metabolic pathways. Shilajit, a herbo-mineral preparation can offer a new and promising approach in the long-term management of maturity onset diabetes mellitus, because of its multifaceted action. Since it can produce a better glycemic control along with improvement in the lipid profile in animals, it is worthwhile to try shilajit either as monotherapy or in combination with other antidiabetic agents clinically. REFERENCES
Copyright 2004 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph04132f2.jpg] [ph04132f1.jpg] [ph04132t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}