 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 37, No. 1, January-February, 2005, pp. 5-12 Educational Forum Chemotherapy of osteoarticular tuberculosis Hazra Avijit, Laha Baisakhi Department of Pharmacology, Institute of Postgraduate Medical Education and Research, 244B Acharya J.C. Bose Road, Calcutta - 700 020
Correspondence Address:Department of Pharmacology, Institute of Postgraduate Medical Education and Research, 244B Acharya J.C. Bose Road, Calcutta - 700 020 Code Number: ph05002 Abstract Tuberculosis (TB) of the bones and joints is rampant in India with the dorsolumbar spine as the most common site of osseous involvement. For diagnosis, clinical suspicion needs to be confirmed through appropriate laboratory and imaging investigations, and increasingly nowadays, nucleic acid amplification techniques. Chemotherapy remains the cornerstone of management complemented by rest, nutritional support and splinting, as necessary. Operative intervention is required if response to chemotherapy is unsatisfactory and for spinal stabilization. The drugs and regimens are fundamentally similar to those for pulmonary TB. However, there is lack of consensus on the appropriate duration of treatment. The prevailing practice of extending treatment till radiological evidence of healing is complete, may be unnecessary in view of recent reports that 6-9 months of therapy is sufficient for the majority of cases. Relapse rates are not drastically improved by extending treatment to 12 months or even longer, except perhaps in pediatric cases. However, prolonged treatment may be required if surgical debridement is indicated but cannot be done. Multidrug-resistant TB should be suspected if disease activity shows no signs of abating after 4-6 months of uninterrupted therapy. These cases are therapeutically challenging and will require second line or experimental antiTB drugs, supported by resistance testing where feasible. Coexistent HIV/AIDS may also necessitate prolonged treatment. Interactions between first line antiTB drugs and antiretroviral medication can complicate matters. Close monitoring is essential in all cases, with dechallenge and cautious reinstitution of drugs in the event of toxicity. While awaiting the arrival of long overdue new antiTB medication, existing drugs and regimens must be used in an informed manner with emphasis on patient compliance. Key Words: Bone tuberculosis, caries spine, antitubercular drugs, MDR-TB Tuberculosis (TB) remains one of the major killer infections worldwide. About 2.2 million new cases of TB occur every year. As per the World Health organization (WHO) 1999 report on global tuberculosis control, South East Asia accounts for approximately 40% - two out of five cases of TB in the world. Within South-East Asia, more than 95% of cases are found in India, Indonesia, Bangladesh, Thailand, and Myanmar. It is estimated that there are about 60 lakh active pulmonary TB cases in India and annual death rate due to TB is about 500,000. Of the various secondary forms of the disease, TB of the bones and joints is a common orthopedic problem in India and in many other developing countries. Indeed, after decades of consistent decline in incidence, a resurgence of TB is occurring in developed countries, partly linked to the prevalence of human immunodeficiency virus (HIV) infection, and this includes osteoarticular TB.[1],[2] Sites of infection and etiopathology In India, the incidence of osteoarticular TB appears to be higher in children, adolescents and young adults, than in the elderly. The spine is probably the most common site of osseous involvement,[2] followed by the hip and knee.[3] Spinal disease is found in about 1% of all TB cases.[4] In the spine, the usual involvement is vertebral bodies and intervertebral disks in the dorsolumbar regions. Less commonly the cervical vertebrae,[5] craniovertebral junction,[6],[7] sacrum[8] and sacroiliac joints may be involved. Atypical presentations of spinal TB, such as intradural spinal TB, may occur and may be misdiagnosed as neoplasm without a high index of clinical suspicion.[9] Other sites of involvement reported in the literature are ribs, pelvic bones, small bones of the foot,[10] long bones,[11] sternoclavicular joint,[12] sternum,[13] calvarial bones[14] and bursae.[15],[16] Multifocal skeletal TB is an uncommon entity but has been reported from India[17] and other countries.[18],[19],[20] The human subtype of Mycobacterium tuberculosis is almost invariably the causative organism in India. The skeletal focus is always secondary to another focus, usually in the lungs or in the mediastinal lymph nodes. The spread is via the blood stream and the infection settles in bone usually near the epiphyseal cartilage in proximity to the synovial membrane. The ′tubercle′ is the microscopic pathological lesion with central necrosis surrounded by epithelioid cells, giant cells and mononuclear cells. Two types of microscopic lesions have been described - (a) the caseating exudative type where caseating necrosis and cold abscess formation predominate, and (b) the proliferating type where cellular proliferation predominates with minimal caseation. The tuberculous granuloma is the extreme form of this type. In children the lesion is commonly of the caseating type with rapid and extensive destruction of bone and cartilage, whereas in adults the proliferating type with less bone destruction is usual. Clinical features and investigations Clinically the onset of TB in any bone or joint is insidious. Constitutional symptoms like low-grade fever, anorexia and weight loss usually precede localizing symptoms and signs such as pain, tenderness and swelling of the affected part. Other local features may be muscle spasms and discharging sinuses. There may be additional features referable to the primary site of involvement, such as the lungs, but these may be minor or even absent. In addition to the usual array of diagnostic tests for TB, advanced imaging modalities such as computerized tomography (CT),[6],[21] magnetic resonance imaging (MRI)[6],[21],[22] and bone scans[19] can be very helpful. Indeed, MRI, with gadolinium enhancement if necessary, is considered an ideal modality for making the diagnosis, demonstrating the extent of disease, identifying complications and assessing response to treatment.[2] It provides better delineation of vertebral lesions with adjoining soft tissue involvement and nerve compressions, than CT. The imaging modalities can guide aspiration cytology and the tissue aspirates can be subjected to smear examination and culture.[21],[23] Biopsy of the bony lesion, synovium or soft tissue masses may be needed to clear up diagnostic confusion.[24],[25] Molecular diagnostic techniques like the polymerase chain reaction (PCR)[26] and other forms of nucleic acid amplification tests are being applied nowadays to tissue samples. Although DNA-based PCR can be quite sensitive, it may not distinguish between viable and non-viable bacilli. Messenger-RNA based reversed transcription PCR may be more specific in this regard. Testing for HIV may also be needed if the clinical circumstances so dictate. General principles of management If osteoarticular TB is diagnosed and treated at an early stage, the large majority of patients are expected to achieve healing with near normal function. The mainstay of treatment is multidrug antitubercular chemotherapy and active or assisted non-weightbearing exercises of the involved joint throughout the period of healing.[27] An initial period of rest is to be followed by supervised gradual mobilization. In caries spine, various types of spinal support in the form of collars, braces and corsets, may need to be used. Adequate nutritional support is also essential, as in all forms of TB. The goals of treatment are to:[28]
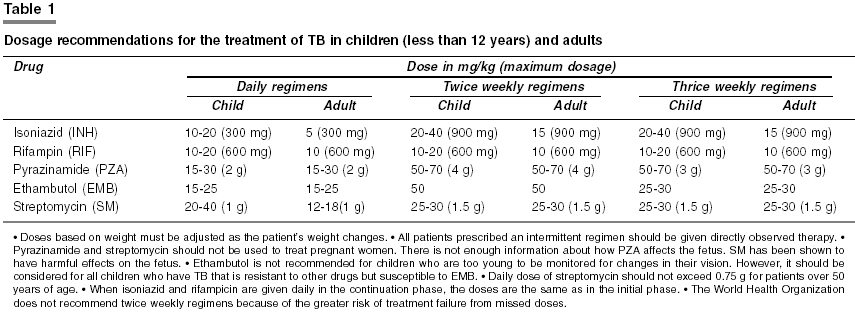
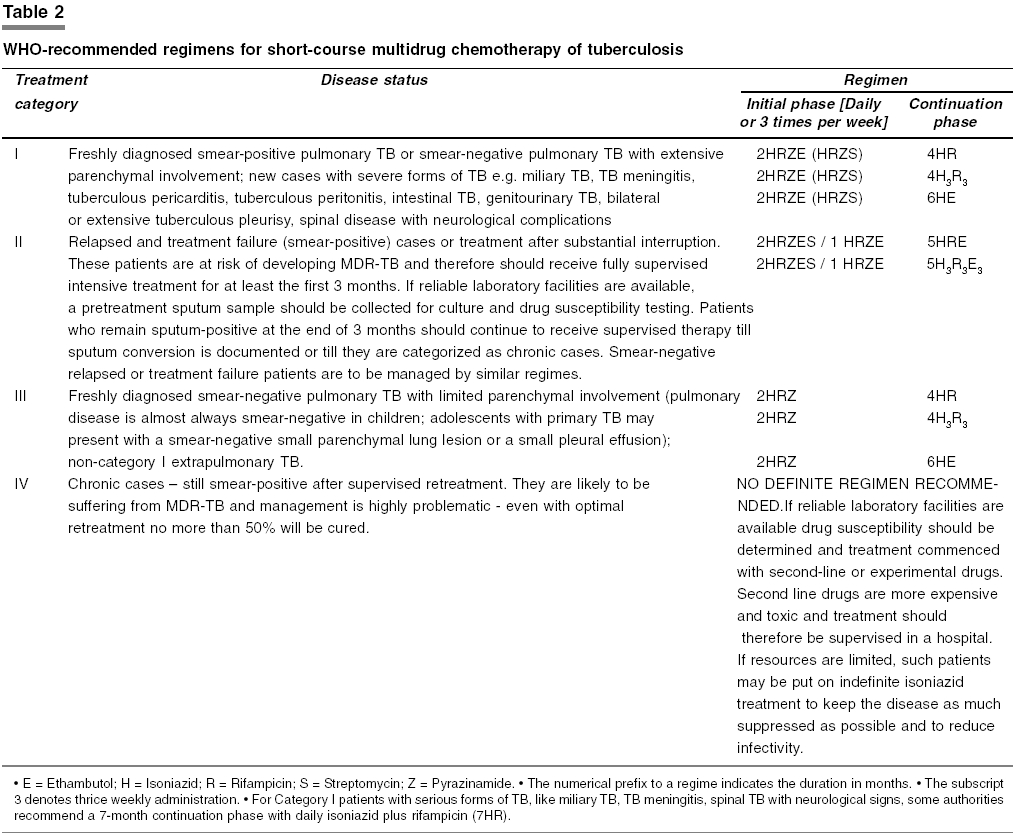
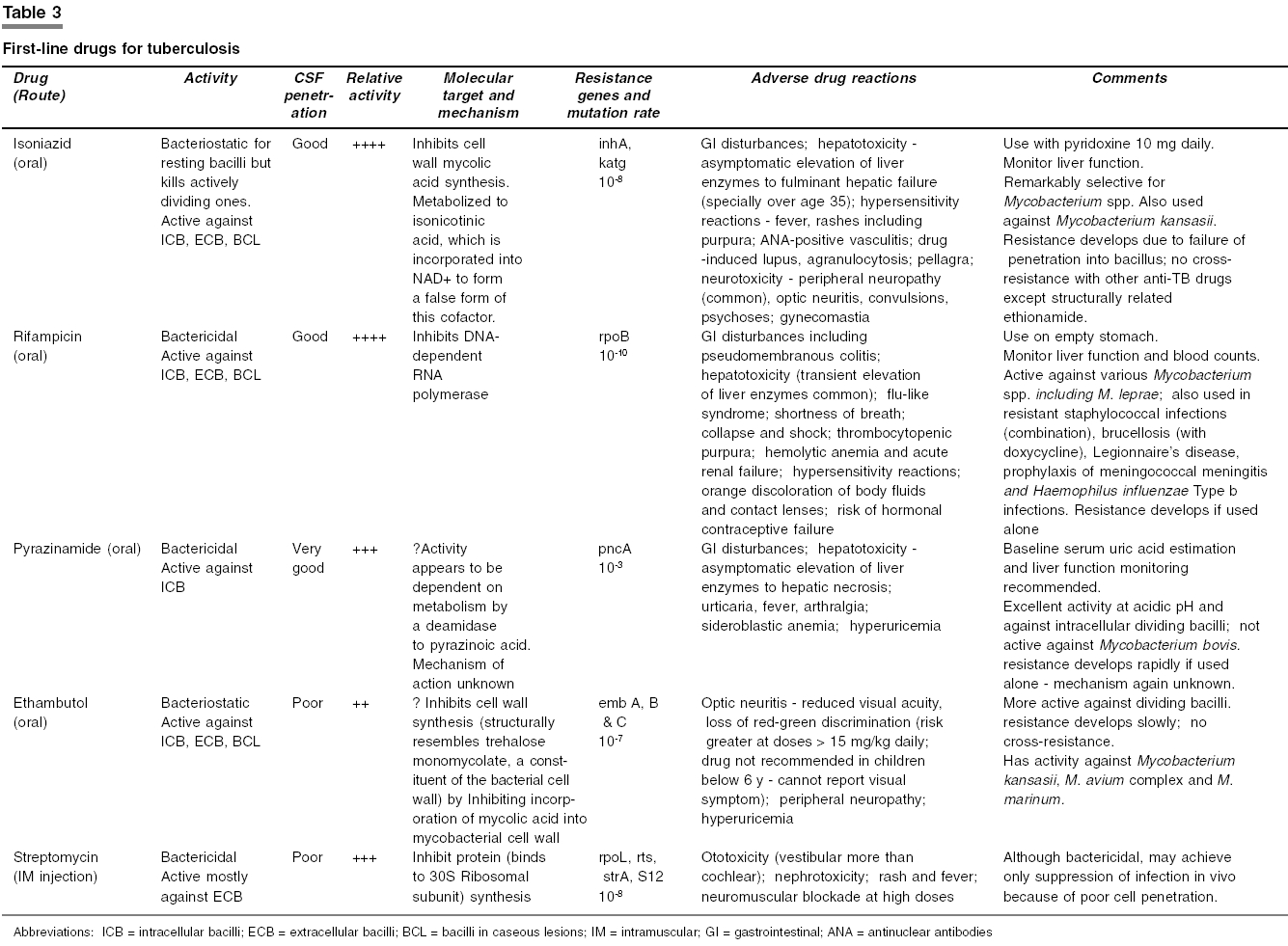
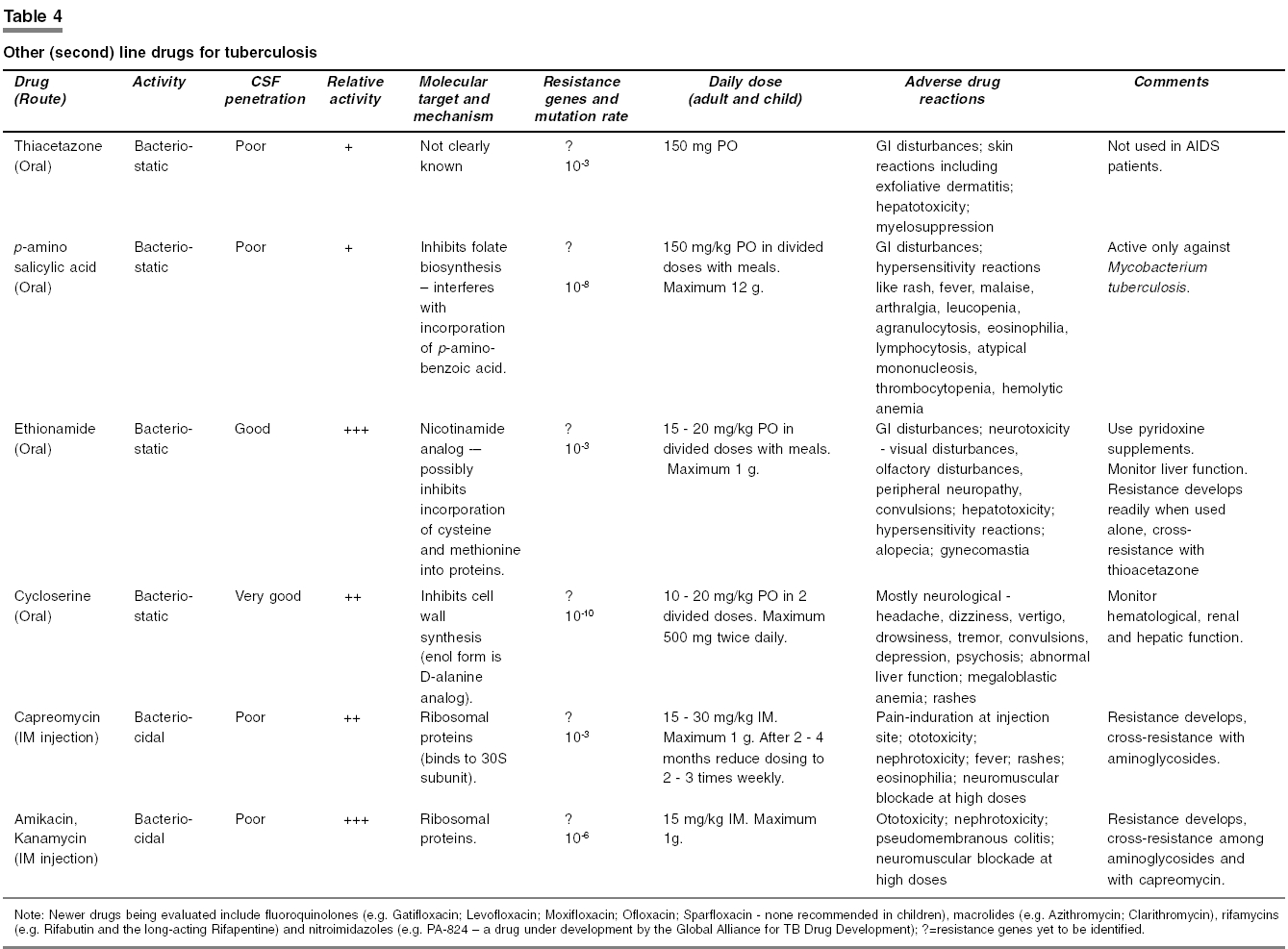
An initial period of hospitalization enables supervised treatment. Continuation treatment can be on a domiciliary basis. However, it is always advisable to follow the principle of directly observed treatment wherever feasible. Intermittent (thrice weekly) regimens have not received adequate trials in skeletal TB. Intermittent regimens, if resorted to for logistical reasons, should be directly supervised. Operative intervention is required when the patient is not responding to an adequate trial of chemotherapy (e.g. synovectomy and debridement); if the therapeutic outcome is not satisfactory (e.g. excisional arthroplasty of the hip or the elbow); or the healed status has resulted in a painful ankylosis (e.g. arthrodesis for the ankle, the wrist, or the knee). It is also required for an unstable spine. Joint replacement can be considered only if the disease process has remained quiescent for at least a year or more. Multidrug resistance should be suspected if the disease activity does not subside after 4 to 6 months of uninterrupted combination chemotherapy.[27] Such patients (an estimated 5-10%) or those unable to tolerate first-line antitubercular drugs require specialist intervention. Principles of antiTB chemotherapy As in other forms of TB, multidrug therapy is the norm in bone and joint TB. Mycobacterium tuberculosis is a complex pathogen. It produces at least 250 distinct enzymes compared to only 50 for Escherichia coli. Mutations capable of conferring drug resistance occur frequently. Multiple drugs used in combination will reduce the possibility of selecting drug-resistant strains and hence chances of relapse. Among the first-line drugs, pyrazinamide, being active in an acidic environment, takes care of the persistent intracellular bacilli. In general, regimens that are adequate for treating pulmonary TB are also effective for treating extrapulmonary TB. The problem lies in deciding on the appropriate duration of treatment for various osteoarticular sites and in selecting appropriate drugs when resistance to the first-line drugs is encountered. The general dosage recommendations for first-line antiTB drugs are presented in For the purpose of rationalizing and initiating treatment, WHO categorizes TB patients into four categories depending upon clinical severity and priority.[29] Treatment in a category is divided into initial, intensive, and subsequent continuation phases. The intensive phase comprises maximum number of drugs given daily (preferably under supervision) and is intended to bring about rapid clinical amelioration and achieve non-infectivity. Treatment is then continued with 2 or 3 drugs given daily or intermittently to eliminate residual bacilli and prevent relapse. These regimens are presented in [Table - 2]. It may be noted that apart from newly diagnosed TB spine patients being placed in Category I, there is no specific categorization of other sites of osteoarticular involvement. [Table - 3] and [Table - 4] summarize the characteristics of standard first-line and current second-line antiTB drugs. Duration of chemotherapy Although the first-line regimens are now standardized, the problem lies in deciding upon the appropriate duration of chemotherapy in osteoarticular TB. This is an area where there is no consensus. WHO categorizes caries spine as a severe form of extrapulmonary TB with new cases assigned to Category I. Therefore, by WHO criteria, all caries spine cases should be treated for a minimum of 6 months. Many surgeons in India prefer to continue treatment till there is adequate radiological evidence of healing, which can take much longer than 6 months. It is a moot point whether treatment really needs to be so long. In various studies, the duration of therapy has varied widely - 6 months in sacral TB,[30] 12-18 months in afflictions of various spinal sites,[5],[31],[32] 12-18 months in TB of craniovertebral junction,[6],[7] 14 -18 months in sternoclavicular joint involvement,[12] 12-20 months in TB affecting the talus,[33],[34] etc. However, certain suggestions can be made from a perusal of the literature:
Treatment in HIV-positive individuals The treatment regimens as outlined above are also effective in the presence of HIV infection. However, HIV-positive patients should be closely monitored and should be re-evaluated if response appears inadequate. Unfortunately, complex interactions between rifampicin and antiretroviral drugs may force withdrawal of conventional regimens. Rifabutin has been used as an alternative to rifampicin in such situations. Treatment of MDR-TB Multi-drug-resistant TB (MDR-TB) is defined as resistance to both isoniazid and rifampicin, with or without resistance to any other antituberculosis drugs. As already stated, resistance to multiple first-line antiTB drugs should be suspected if disease activity does not show signs of subsiding after 4-6 months of uninterrupted multidrug therapy.[27] Many crucial management issues in MDR-TB treatment remain unanswered and the existing primary literature consists almost entirely of retrospective cohort studies.[39],[40] There are no standardized regimens or guidelines. Second-line and potential antitubercular drugs will have to be tried. If reliable laboratory facilities are available, drug susceptibility should be determined and treatment commenced with relevant second-line or experimental drugs. It has been suggested that four or five (at least three) antitubercular drugs, including the fluoroquinolones, must be included in the regimen and that, if needed, these drugs should be changed at the same time, not one by one.[41] Further, treatment with these drugs takes 2 years or longer, as opposed to 6 to 9 months with isoniazid-rifampicin-containing regimens.[42],[43] However, studies have also reported reasonably satisfactory responses in shorter periods through regimens incorporating fluoroquinolones like ofloxacin and sparfloxacin.[44],[45],[46] In general, second-line drugs are more expensive and toxic and treatment, at least in the initial part, should therefore be supervised in a hospital. Therapeutic drug monitoring has been employed.[47] Immunomodulatory therapy with levamisole and Mycobacterium vaccae has been disappointing. Other immunomodulators, such as recombinant human interleukin-2 and recombinant interferon-alpha2b, are being tried.[48],[49] Unfortunately, no separate guidelines exist for managing multidrug-resistant osteoarticular TB. In the event of toxicity[50] As evident from [Table - 3] and [Table - 4], a number of adverse drug reactions are possible from the use of antiTB drugs. If a reaction occurs but its nature does not single out a particular drug, cautious rechallenge is the only way to identify the offending drug or drugs; starting with the one least likely to be responsible for the symptoms. Rechallenge is started with one drug in a small challenge dose, which is increased stepwise to full therapeutic dose over a few days. This procedure is repeated, with one drug added at a time. The step-up should be even more gradual if the initial reaction is severe. Needless to say that if the reaction recurs, the offending drug has been identified, it must be withdrawn. Combination tablets are not suitable for this purpose and rechallenge should not be attempted if the patient is uncooperative or if a close watch is not possible. Any reaction to thioacetazone, even if it is simple itching, should prompt immediate withdrawal of the drug and rechallenge should not be attempted with this drug. Treatment may be continued by replacing the offending drug with a suitable alternative, or with a reduced number of drugs if none is suitable. Specialist advice may be sought. It is also noteworthy that the resumed regimen is considered to be a new start to the treatment. This prolongs the duration of therapy but, on the other hand, reduces the chance of recurrence. Most antiTB drugs, particularly pyrazinamide, rifampicin, and isoniazid, can cause hepatotoxicity, while ethambutol is seldom responsible. If a patient on antiTB drugs develops hepatitis, and no other cause is likely, drug-induced hepatitis must be presumed and the drugs stopped. Once the hepatitis has resolved, the same regimen may be cautiously reintroduced. If the hepatitis has been severe, then it is probably safer to avoid pyrazinamide, and possibly also rifampicin, altogether. An alternative regimen in such patients can be a 2-month initial phase of daily isoniazid, ethambutol and streptomycin followed by a 10-month continuation phase of isoniazid plus ethambutol. A severely ill TB patient with drug-induced hepatitis may die without antiTB treatment. In this case the patient may be treated with the two least hepatotoxic drugs, namely streptomycin and ethambutol instead of interrupting TB treatment. Isoniazid may be cautiously reintroduced after the hepatitis has resolved. Follow-up and prognosis Chemotherapy in osteoarticular TB not only helps to control the infection per se but timely surgery can also be done safely, if efficient conservative treatment is carried out in the first instance with rest and chemotherapy. Whatever the goal the importance of regular follow-up to assess disease activity and to ensure patient compliance cannot be overemphasized.[51] Supervised drug treatment programs will facilitate the latter. The diagnosis of quiescence is as important as the diagnosis of the lesion itself and has to be judged through clinical (local and systemic), radiological and laboratory criteria. The prognosis in general is good with adequate treatment regimens sustained for an appropriate length of time. In some series children appear to fare better than adults.[52] In spinal TB, established deformity and neurological deficits are more difficult to reverse,[21],[52] which points to the importance of stabilization surgery. Conclusion TB continues to kill approximately two million people each year around the globe. Yet, according to WHO estimates based on 2001 data, worldwide, only 30% of active TB cases are being diagnosed and treated under directly observed therapy, short-course (DOTS) programs. The global targets of 70% case detection and 85% cure rates for those detected must be reached by 2005 in order to halve TB prevalence and deaths by 2010. The opportunity provided by the World TB Day (March 24) should be taken for increasing awareness of various stakeholders on the importance of effective TB control and for social mobilization. On the chemotherapy front, we continue to fight with the available drugs against the formidable challenges posed by MDR-TB and the HIV-TB vicious cycle. It is sad but true that there have been no new antitubercular drugs for at least the past three decades. However, the Global Alliance for TB Drug Development has been set up and is committed to delivering its first new drug by 2010. The total funding is expected to exceed US$ 150 million. The Alliance also seeks to make antiTB drugs available, particularly in the countries worst hit by the disease, at prices that are affordable to their populations. Cost-effective new antiTB drugs are badly needed to shorten the duration of TB treatment, simplify the regimens, improve the treatment of latent TB infection and overcome the resilience of MDR-TB. Till then we must continue to apply existing drugs and regimens in an informed manner with the maximum emphasis on patient adherence to treatment. References
Copyright 2005 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph05002t4.jpg] [ph05002t3.jpg] [ph05002t2.jpg] [ph05002t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}