 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 37, No. 1, January-February, 2005, pp. 40-43 Research Letter Self-medication among urban population of Jammu city Sharma R, Verma U, Sharma CL, Kapoor B Departments of Pharmacology and Therapeutics, Govt. Medical College, Jammu
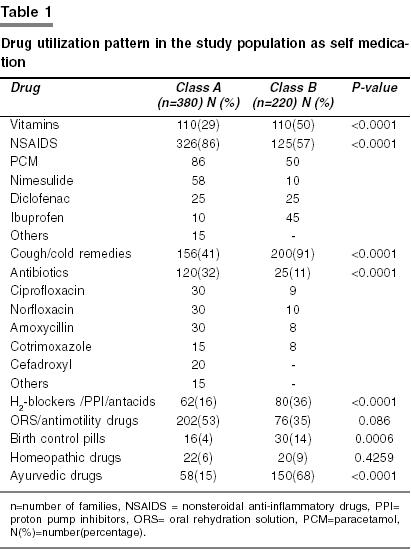
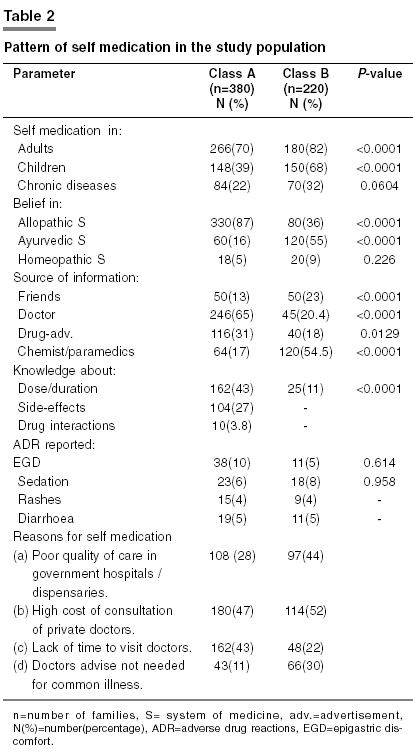
Correspondence Address:Departments of Pharmacology and Therapeutics, Govt. Medical College, Jammu Code Number: ph05011 Sir, Self-medication can be defined as obtaining and consuming drugs without the advice of a physician either for diagnosis, prescription or surveillance of treatment.[1] There is a lot of public and professional concern about the irrational use of drugs. In developing countries like India, easy availability of a wide range of drugs coupled with inadequate health services result in increased proportions of drugs used as self medication compared to prescribed drugs.[2] Although, OTC (over the counter) drugs are meant for self medication and are of proved efficacy and safety, their improper use due to lack of knowledge of their side effects and interactions could have serious implications, especially in extremes of ages (children and old age) and special physiological conditions like pregnancy and lactation.[3],[4] There is always a risk of interaction between active ingredients of hidden preparations of OTC drugs and prescription medicines, as well as increased risk of worsening of existing disease pathology. As very few studies have been published regarding self medication pattern in our community, therefore, we conducted this cross-sectional study in 600 urban families living in Jammu city to evaluate their self medication practices. Nuclear families were selected randomly by stratified sampling and Jammu city was arbitrarily divided in 10 sections and 60 families were randomly selected from each section. The families under study were further classified into two classes; class-A with head of the family having qualification more than 12th standard and class-B with qualification less than 12th standard. A family having another member with qualification more than 12th standard was also included in the class-A even if the head was not qualified up to the 12th standard. 380 families were included in class-A and 220 families in class-B. A simple questionnaire was prepared and each family was interviewed only once in the local language. At least two members of the family (including head of the family and excluding children below 12 years and mentally sick persons) were interviewed together after obtaining their consent. The questionnaire was filled by a qualified assistant. The questionnaire contained the questions pertaining to identifications data (name of head of the family, number (no.) of children, no. of adults, address, qualifications, employment, income), practice of self medication by the family, commonly used drugs as self medication, knowledge of the family regarding dose, duration, side effects and interactions of the drugs in use, source of information about the drug, attitude towards allopathic, ayurvedic and homeopathic medicines and a recall period of one year was kept. In the end of the study all the data was collected and analysed [Table - 1] and [Table - 2]. All the parameters were compared between class-A and class-B using Chi-square test and P values <0.05 were considered statistically significant. A trend towards self medication in adults was seen both in class-A and class-B. However, use of self medication was significantly more in class-B than class-A [Table - 2]. Previous studies have shown the prevalence of self-medication as 37% in urban population and 17% in rural population in India;[5] where as 12.7% to 95% in other developing counteries.[2],[6],[7] In class-A NSAIDS (non-steroidal antiinflammatory drugs) were widely administered as self medication followed by ORS (oral rehydration solution) /antimotility drugs, cough/cold remedies and antibiotics; whereas, cough and cold remedies were widely used drugs in class-B followed by NSAIDS, vitamins, ayurvedic drugs, H2 blockers/proton pump inhibitors/antacids and ORS/antimotility drugs. Present study also indicated low knowledge about dose/duration, side effects and interactions of commonly used drugs both in class-A and class-B in accordance with reports of the previous studies.[8],[9] Their knowledge about the above parameters was extracted by asking direct questions or indirectly by enquiring about the drug use in sub-therapeutic dose for inadequate period or over use of drugs, use of drugs with a potential to aggravate the existing pathology for which it is used (NSAIDS for epigastric pain, use of cold and cough remedies containing sympatho-mimetic drugs by hypertensive and diabetic patients, use of antimotility dugs for diarrhea/dysentry in children, use of hormonal pills by hypertensive or diabetic women) and concomitant use of drugs with potential interactions (NSAIDS and antihypertensive drugs or iron /calcium preparations and antimicrobials or irrational drug combinations). However, the knowledge regarding dose/duration of drug therapy, adverse drug reaction and drug interaction was significantly more in class-A than class-B. Even in developed countries like USA, it has been seen that the misuse of non-prescription drugs causes tens of thousands of unnecessary hospitalizations each year.[10] In a drug utilization study in USA, it was found that medications that are contraindicated in pregnancy were used at unexpectedly high rate as OTC drugs in obstetric population.[11] There was a trend towards use of ayurvedic and homeopathic drugs in both class-A and class-B for chronic illnesses like joint pains, acid peptic disease, bronchial asthma, obesity, impotence, baldness and female infertility. Moreover, herbs and homeopathic drugs were considered safe and devoid of adverse effects, but the risk of possible drug interactions is always with their use.[12] However, no serious side effect was reported with drugs used as self medication except for few episodes of epigastric discomfort, sedation, rashes and diarrhea with the use of NSAIDS, cough and cold remedies and antibiotics respectively in both the classes. In the present study doctors were found to be the most common source of drug information in class-A where as paramedics/chemists were the most common source of drug information in class-B. These are in concordance with earlier reports.[13],[14] Drug advertisements were also an important source of drug information. Although, patient′s use of advertised medicines could have important health benefits if used appropriately in the early stages of disease, many advertised products are ′lifestyle drugs′, symptomatic treatments and may relieve only the discomfort and are likely to result into increased complications and hospital admissions as a result of uncontrolled disease pathology. Studies of pharmaceutical practice in India have called attention to the role played by pharmacists and pharmacy attendants in fostering self-medication and medicine experimentation among the public.[15] It is argued that the economic rationale and the symbiotic relations that exist between doctors, medical-representatives, medicine wholesalers and retailers, need to be more closely scrutinized by those advocating rational drug use. Patient satisfaction with the healthcare provider, cost of the drugs, educational level, socioeconomic factors, age and gender are the important factors influencing self-medication.[16] Our study clearly indicated the variation in self medication pattern with education status. However, we could not consider the socioeconomic variations in our study, because of difficulty in assessing the true income of the family due to varied and multiple sources of income of majority of the families. Moreover, failure on our part to consider age and gender variations was due to non-availability of all the members at the time of interview, which could be considered as lacuna of our study. However, respondents were very cooperative and answered all the questions in detail. The most common reason for indulging in self medication was given high cost of private doctor′s consultations in both the classes [Table - 2]. Our study presented self medication pattern in a set of urban population, but the condition could be more worst in rural or remote corners of India, where the people are deprived socially, economically and educationally with scarce health facilities. Self-medication, using non-prescription drugs, could be beneficial to patients, healthcare professionals, the pharmaceutical industry and governments, provided these drugs are used rationally. Apart from community education, safety and efficacy of OTC drugs must be assured, so that these products could be safe even in the event of improper use. For registration as an OTC drug, specific efficacy trials may be conducted in real self-medication situation. FDA has strongly advocated that labeling of the OTC drugs should be easy to understand by the consumer and should contain the list of active ingredients, warnings, directions and inactive ingredients.[10] Easy availability of wide range of drugs without prescription of registered practitioner in our country is the major factor responsible for irrational use of drugs as self medication, thus resulting into impending health problems(antimicrobial resistance, increased load of mortality and morbidity) and economic loss. The need for promoting appropriate use of drugs in health care system is not only because of the financial reasons with which policy makers and manager are usually most concerned, but also for health and medical care of patients and the community. There is need for authorities to make the existing laws regarding OTC drugs strong to ensure their rational sale and use. Moreover, specific pharmacovigilance is needed and the patient, pharmacist and physician must be encouraged to report any adverse events. Periodic studies on the knowledge, attitude and practice of self medication may give insight into the changing pattern of drug use in societies. Anexure 1 Questionnaire used for assessing pattern of self-medication.
References
Copyright 2005 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph05011t2.jpg] [ph05011t1.jpg] |
| |||||||||

{kind=link}
{kind=link}