 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
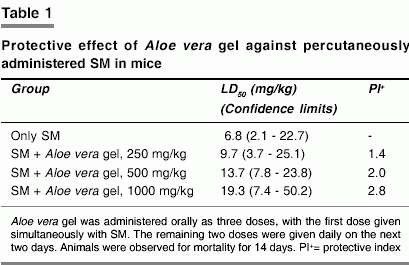
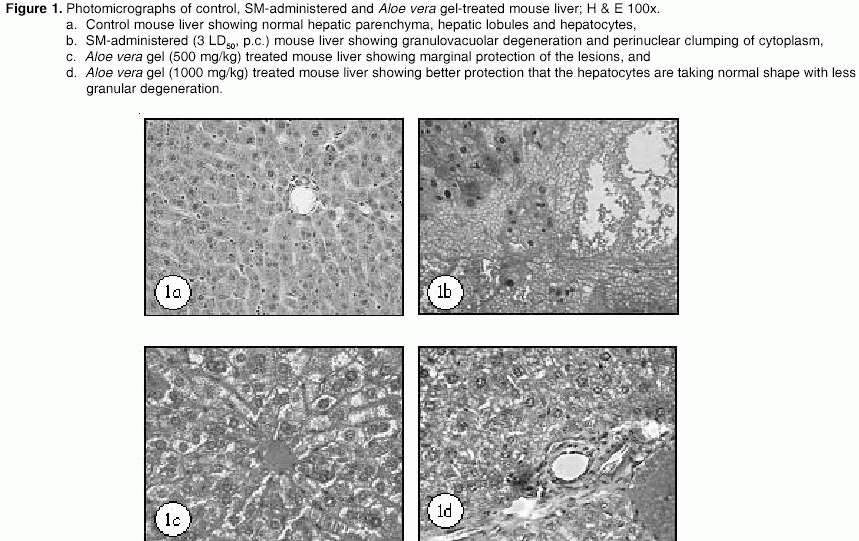
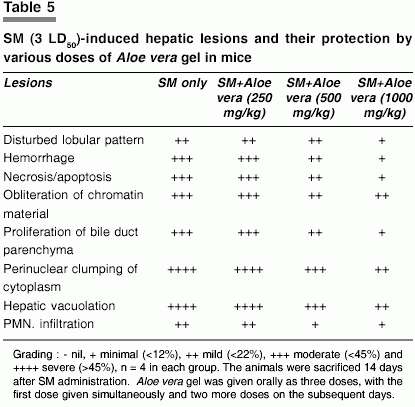
Indian Journal of Pharmacology, Vol. 37, No. 2, March-April, 2005, pp. 103-110 Research Paper Protective effect of Aloe vera L. gel against sulphur mustard-induced systemic toxicity and skin lesions Anshoo G., Singh S., Kulkarni A.S., Pant S.C., Vijayaraghavan R. Defence Research and Development Establishment, Gwalior - 474 002 Code Number: ph05019 ABSTRACT OBJECTIVE: Sulphur mustard (SM), chemically 2,2'-dichloro diethyl sulphide, is an incapacitating and extremely toxic chemical warfare agent, and causes serious blisters on contact with human skin. SM forms sulphonium ion in the body that alkylates DNA and several other macromolecules, and induces oxidative stress. The aim of this study was to evaluate the protective effect of Aloe vera L. gel against SM-induced systemic toxicity and skin lesions.MATERIALS AND METHODS: Aloe vera gel was given (250, 500 and 1000 mg/kg) orally to mice as three doses, one immediately after SM administration by percutaneous route, and the other two doses on the next two days. Protective index was calculated with and without Aloe vera gel treatment. Aloe vera gel was also given orally as three doses with 3 LD50 SM and the animals were sacrificed for biochemical and histological evaluation, 7 days after SM administration. In another set of experiment Aloe vera gel was liberally applied on the SM administered skin site and the animals were sacrificed after 14 days to detect its protective effect on the skin lesions induced by SM. RESULTS: The protection given by Aloe vera gel was marginal. 1000 mg/kg dose of Aloe vera gel gave a protection index of 2.8. SM significantly decreased reduced glutathione (GSH), oxidised glutathione (GSSG) and WBC count, and significantly increased malondialdehyde (MDA) level, RBC count and Hb concentration. Aloe vera gel offered protection only in the increase of MDA level by SM. Severe damage was observed in the histology of liver, spleen and skin following SM administration, and 1000 mg/kg of Aloe vera gel partially protected the lesions. However, topical application of Aloe vera gel showed better protection of the skin lesions induced by SM. CONCLUSION: The study shows that percutaneous administration of SM induces oxidative stress and oral administration of Aloe vera gel could only partially protect it. Topical application of Aloe vera gel may be beneficial for protecting the skin lesions induced by SM. INTRODUCTION Bis (2-chloroethyl) sulphide, is commonly known as sulphur mustard (SM) or mustard gas, is an alkylating agent that causes painful blisters on contact with human skin. It is a frequently used chemical warfare agent and several reports of its use are available.[1] SM forms sulphonium ion in the body which leads to DNA strand break and cell death.[2] Due to the high electrophilic property of the sulphonium ion, SM binds to a variety of cellular macromolecules.[3] Eyes, skin and the respiratory tract are the principle targets of SM toxicity.[2],[4],[5] Because of its high lipophilic property, it rapidly penetrates into the skin. Dermal contact of SM causes erythema, severe itching, blisters and ulceration. There are also several reports that systemic toxicity of SM leads to oxidative stress.[6],[7] Aloe vera (Linn), also known as Aloe barbadensis of family Liliaceae is widely distributed in Asia, Africa and other tropical areas. It has been used in folk medicine for the treatment of skin ailments including wounds and burns, asthma and has recently been investigated for its antioxidant effect.[8] Popular interest and use of Aloe gel preparation has increased dramatically in the last decade. The mucilaginous gel from parenchymatous cells in the leaf pulp of Aloe vera is incorporated in ointments, creams, lotions and other preparations essentially for topical use. There are conflicting reports concerning the efficacy of such preparations.[9],[10],[11] In this study the dermal application of Aloe vera gel as a protective natural product against SM-induced skin lesions, and oral administration as an antioxidant for the systemic toxicity of SM has been evaluated. MATERIALS AND METHODS Chemicals Extreme care was taken during the synthesis of SM in the declared facility of the Defence R & D Establishment. The synthesized SM was found to be more than 99% pure by gas chromatographic analysis. The dilution of SM and its administration to animals was carried out in fume hoods with the personnel wearing butyl gloves. The animals were kept in a well-ventilated area for 48 h,after SM administration and then transferred to the experimental animal room for further monitoring. Polyethylene glycol (PEG-300) was purchased from Fluka Biochemica (USA). The rest of the chemicals were purchased from Merck India Ltd. Aloe vera gel was purchased from the trade and certified by the Indian Aloe Science Council (Safed Musli farms, Gwalior). Animals Randomly bred Swiss female mice (25 to 30 g, body weight) from the Defence R & D Establishment′s animal facility were used for the study. The animals were kept in polypropylene cages on dust-free rice husk as the bedding material. Free access to food (standard pellet diet, Amrut Ltd, India) and water was allowed until two hours before the experiment. The care and maintenance of the animals was as per the approved guidelines of the Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA), India. All animal procedures were approved by the Animal Ethical Committee of the Establishment. A day before percutaneous exposure of SM, the hair on the back of the animals was closely clipped by a pair of scissors. Protection studies against SM-induced lethality SM was administered percutaneously (topical application) in varying doses and Aloe vera gel was administered orally as three doses. The first dose was given simultaneously with SM and the remaining two doses were given daily on the next two days. Three different doses of Aloe vera gel were used (250, 500, 1000 mg/kg, body weight) by dissolving the gel in distilled water. SM was diluted in polyethylene glycol (PEG 300) and applied on the back of the mice. The dilutions were made in such a manner that the quantity applied was not more than 100 µl. Protection was expressed in terms of protection index, which is the ratio of the LD50 with treatment to that of LD50 without treatment. For the determination of each LD50, 3 to 4 log doses were used, and for each dose 4 animals were used. The animals were weighed daily and observed for mortality for a 14-day period. LD50 was determined as per the moving average method.[12] Protection studies against SM-induced oxidative stress To evaluate the protective effect of Aloe vera gel on oxidative stress markers, the following groups of four mice each were utilized. I Distilled water, p.o. + PEG 300 dermal (control group) II Distilled water, p.o. + SM, 3 LD50 (19.4 mg/kg) in PEG 300 III Aloe vera gel (250 mg/kg), p.o. + SM, 3 LD50 (19.4 mg/kg) in PEG 300 IV Aloe vera gel (500 mg/kg), p.o. + SM, 3 LD50 (19.4 mg/kg) in PEG 300 V Aloe vera gel (1000 mg/kg), p.o.+ SM, 3 LD50 (19.4 mg/kg) in PEG 300 SM was diluted in polyethylene glycol (PEG 300) and applied on the back of the mice (percutaneous). The dilutions were made in such a manner that the quantity applied was not more than 100 µl. Aloe vera gel dissolved in distilled water was administered orally as three doses. The first dose was given simultaneously with SM and the remaining two doses were given daily on the next two days. Seven days post SM application the animals were anaesthetized with ether for the collection of blood from the orbital plexus and then killed by cervical dislocation. The liver was dissected out and cleaned for the biochemical estimations and for histology. Spleen and skin samples were also taken out for histological examination. Lipid peroxidation was studied by measuring the formation of thiobarbituric acid reactive substances according to the method of Buege and Aust.[13] One hundred milligram of liver tissue was directly homogenized in 5 ml thiobarbituric reagent and boiled for 30 min. The content of the tube was cooled and centrifuged. Optical density of clear supernatant was measured at 535 nm in a spectrophotometer. The amount of MDA formed was calculated, using a molar extinction coefficient of 1.56 X 105 M-1cm-1 and expressed as nmol/gm of tissue. Glutathione concentration of tissue was assayed by Hisin and Hilf fluorometric method.[14] One hundred and fifty milligram of tissue was homogenized in 0.1 M sodium phosphate EDTA buffer (pH 8.0) and 25% meta phosphoric acid was added. The content of the tube was centrifuged and supernatant was used for GSH and GSSG estimation. Analysis of hematological variables viz., WBC count, RBC count, Hb concentration were carried out using a hematocytometer, Beckman Coulter Analyser. All the values are expressed in terms of percentage change as compared to healthy control group. Protection studies against SM-induced histopathology Liver, spleen and skin samples were fixed in 10 % neutral buffered formalin solution. After proper fixation, small pieces were processed by dehydration and embedded in paraffin wax. Sections of 5-6 µm thickness were prepared and stained with hematoxylin and eosin for light microscopy.[15] From each sample ten slides were prepared (Total 40 slides for 4 animals). Out of 40 slides, six slides were selected randomly for lesion evaluation. From each selected slide, 9 µm[2] area was identified randomly and lesions were marked and compared with that of control. The severity of the lesions was characterized using LEICA - Qwin - 500 Image Analyser and converted into percentage. Protection studies against SM-induced skin lesions To evaluate the protective effect of Aloe vera gel on SM-induced skin lesions a separate study was carried out. SM was diluted in acetone and applied on the back of the mice (5 mice per group). Two doses of SM were used, 5 mg/kg and 10 mg/kg. After 24 h Aloe vera gel was applied liberally once daily for 14 days, the animals were sacrificed and skin samples were dissected out for histological examination as explained above. Statistical analysis All the variables were analyzed by one-way ANOVA with Dunnett′s multiple comparison procedure. A probability of < 0.05 was considered as statistically significant. RESULTS The LD50 of SM in PEG-300 through the percutaneous route in mice was found to be 6.8 mg/kg when the animal mortality was recorded till 14 days of SM administration. Oral Aloe vera gel gave a dose-dependent protection against SM. A dose of 1000 mg/kg of Aloe vera gel gave 2.8-fold protection [Table - 1]. The body weight of the animals administered with 3 LD50 (19.4 mg/kg) of SM, decreased progressively. Body weight of the animals in the SM group was significantly decreased compared to the control group from one day after administration and was significantly decreased in all the groups on 7 days after administration. The body weight was 61.3±1.9% after 7 days in the SM group. Aloe vera gel failed to protect the decrease in body weight even at 1000 mg/kg dose [Table - 2]. Percutaneous administration of SM insignificantly decreased the WBC count and significantly increased the RBC count and the hemoglobin content [Table - 3]. Oral administration of Aloe vera gel failed to protect the changes induced by SM even at 1000 mg/kg dose. SM also significantly decreased GSH and GSSG content. Seven days after SM administration (3 LD50), the GSH and GSSG contents were 38.4±0.4 % and 38.6±2.4 % respectively. Oral administration of Aloe vera gel failed to protect the depletion of GSH and GSSG caused by SM even at 1000 mg/kg dose. The MDA content was significantly increased after SM administration. There was some improvement in the MDA level after treatment with Aloe vera gel [Table - 4]. SM caused severe damage to the liver, spleen and the skin (site of application). The liver of control mice showed normal hepatic cord arrangement, hepatic lobes and hepatocytes with normal hepatic parenchyma [Figure - 1]a. Following SM application, liver histopathology exhibited granulovacuolar degeneration of hepatocytes and perinuclear clumping of cytoplasm. Varying degree of necrosis was observed in the hepatocytes. Hepatic parenchyma also revealed significant fatty changes [Figure - 1]b. Treatment with 250 mg/kg of Aloe vera gel orally did not protect the hepatic lesions and 500 and 1000 mg/kg Aloe vera gel provided marginal protection to these lesions. The hepatocytes were of normal shape, yet granulovacuolar degeneration of cytoplasm still persisted [Figure - 1]c and d. Perinuclear clumping of cytoplasm and bile duct proliferation were still observed even after treatment with 1000 mg/kg of Aloe vera gel. A comprehensive account of various histopathological lesions in the hepatic tissue and their protection by Aloe vera gel is given in Table 5. Histological features of spleen from control mice showed normal histoarchitecture with white pulp consisting of lymphatic follicles and red pulp consisting of sinusoids and other elements of blood [Figure - 2]a. Spleen of SM-applied mice showed reduced density of white pulp follicles and congestion in red pulp. The red pulp was also infiltrated with macrophages. Obliteration of marginal zone and degeneration of peri arteriolar lymphatic sheath (PALS) was also observed following percutaneous administration of SM [Figure - 2]b. Treatment with 250 mg/kg of Aloe vera gel orally, did not give any protection and 500 mg/kg gave minimal protection to SM-induced splenic lesions [Figure - 2]c). However, 1000 mg/kg Aloe vera gel treatment gave protection as evidenced by reorganization of white pulp follicle cells and the germinal center [Figure - 2]d. A comprehensive account of various histopathological lesions in the splenic tissue and their protection by Aloe vera gel is given in Table 6. The histology of control mouse skin showed three distinct layers viz., epidermis, dermis and hypodermis. The epidermis consisted of three visible layers (i) the dark stained corneum layer having flattened dead cells, (ii) the stratum granulosum comprising dense basophilic granular cells and (iii) the stratum spinosum consisting of large polyhedral cells. The dermis consisted of two layers of connective tissue, a superficial papillary and deeper reticular layer [Figure - 3]a. Percutaneous application of SM in mice caused severe epidermal atrophy as evidenced by extensive epidermal necrosis in the stratum corneum layer. Spinous cells were swollen, enlarged and vacuolated, and prominent dermoepidermal separation was also observed. A large number of inflammatory cells were observed in the dermal region. The degenerated dermoepidermal region was covered by exudates composed of fibrin, leucocytes and RBCs [Figure - 3]b. Oral administration of Aloe vera gel 250 mg/kg did not protect SM-induced skin injury. Oral administration of 500 and 1000 mg/kg Aloe vera gel reduced the skin lesions as skin histology showed reepithelization, reduced number of inflammatory cells and dermoepidermal gaps [Figure - 3] c and d. There was a significant improvement in the lesions caused by SM by the topical application of Aloe vera gel [Figure - 4]d. The reepithelization was better and the gaps were also reduced. DISCUSSION The probability of accidental exposure to lethal concentrations of SM exists during its decontamination program by the declared State Parties, as part of the directive of the Organization for the Prohibition of Chemical Weapons (OPCW, The Netherlands). Keeping this point in view, mice were exposed to SM by the percutaneous route which is closer to the actual conditions, and the protection of Aloe vera gel against SM toxicity was evaluated. Following SM administration the animals generally died within a period of 14 days.[16] The efficacy of Aloe vera gel was evaluated against SM toxicity and maximum protection was observed with1000 mg/kg oral dose. Oxidative stress is defined as a disturbance in the pro-oxidant and antioxidant balance, in favor of the pro-oxidant state. Percutaneous (dermal) administration of SM can induce oxidative stress in the experimental animals and antioxidants can protect it to some extent.[6],[7],[17] The alternative hypothesis for SM toxicity is related to GSH which may act as an intracellular scavenger for SM.[6],[7],[18] A significant depletion of GSH was observed in the present study also. GSH has an important function in protecting the cell from oxyradicals and reactive chemicals. It scavenges free radicals and its depletion is related to cytotoxicity. It is also possible that in the absence of GSH the partially reduced oxygen species may be transformed into highly toxic oxidants, which may further react with membrane phospholipids initiating lipid peroxidation. Since Aloe vera gel was giving marginal protection against the lethality of SM, oxidative stress markers were evaluated. Oral administration of Aloe vera gel did not show recovery of GSH and GSSG, but the elevation of MDA level was protected, showing marginal protection against SM-induced toxicity. Significant protection on GSH, GSSG and MDA was observed following SM toxicity only when the protection as measured in terms of protection index was very high.[6],[7] Since the maximum protection index obtained in the present study was 2.8 at 1000 mg/kg dose of Aloe vera gel, GSH and GSSG were not protected. The marginal protection offered by Aloe vera gel may be due to the active components aloesin, aloeresin, and aloin.[8] But Aloe vera gel has been found to be beneficial in protecting the reduction of GSH and increase in MDA following gamma radiation.[19] Following percutaneous administration of SM the animals lost weight progressively and appeared extremely weak and emaciated. Hemoconcentration was also observed. It is generally expected that following SM administration there should be a profound decrease in WBC count. But, due to hemoconcentration the decrease in WBC count following SM administration is not significant. Hemoconcentration occurring due to the increased permeability of the endothelial cells of the blood vessels may be the reason for the increased RBC count and Hb content. Lipid peroxidation is attributed to the increased permeability. Since the protection offered by Aloe vera gel was only marginal there was no significant protection in the hematological variables. SM is a potent alkylating agent and causes serious blisters on contact with human skin. Topical application of SM causes erythema, followed by blisters and ulceration. In the animal model percutaneously administered SM is extremely toxic.[20] Though apparent blisters were not observed in animal models, ulceration appeared after 14 days of dermal application of SM. Because of its lipophilic properties, SM rapidly penetrates the skin and the best method of minimizing the toxic effects on the skin as well the systemic toxicity is by decontamination. The presently used decontaminants are Fuller′s earth, a physical decontaminant and CC2 suspension, a personal-chemical decontaminant.[21],[22] Even a shortest contact period of SM on the skin is sufficient for the blister formation. The presently used medical methods for the treatment of blisters are the application of petroleum jelly, antimicrobial ointments or povidone-iodine containing ointment which are symptomatic measures.[23],[24] The mechanism of wound healing occurs in three stages; inflammation, proliferation and remodelling. The wound healing process depends on the local blood circulation, as well as the formation and deposition of collagen. Aloe vera gel contains important constituents necessary for wound healing, such as ascorbic acid, tocopherols, amino acids, and Zinc.[25] Ascorbic acid enhances the synthesis of collagen and counterbalances collagen breakdown. Tocopherol is a fat-soluble vitamin found in Aloe vera gel, that has proven antioxidant activity. It stabilizes lysosomal enzymes needed for the synthesis of collagen and scavenges free radicals that may interfere in the wound healing process. Zinc improves the tensile strength and improves wound healing.[26] Aloe vera gel reduces dehydration and necrosis, and also dilates the capillaries. Another expected mechanism of Aloe vera gel for wound healing is the mannose-containing product which increases macrophage activity and fibroblast proliferation.[26] When SM is diluted in PEG-300 and applied topically the systemic toxicity is more than the local skin lesions due to the combined lipophilic characteristics of SM and PEG-300. Hence to induce a prominent skin lesion SM was diluted in acetone which is a less lipophilic solvent with a better spreading effect. When PEG-300 is used as a solvent no erythema is observed and the lesions develop only after 14 days. While in acetone, erythema develops in two days and the lesions also appear in about 7 days. SM-administered mice skin showed invasion of the epidermis by acute inflammatory cells, dermoepidermal separation, erosion of dermis and accumulation of exudates composed of fibrinoid material. An increased number of polymorphonuclear cells were also observed in guinea pig skin administered with liquid SM.[27] In the present study topical application of Aloe vera gel protected the skin lesions and they were less severe. As Aloe vera gel stimulates and enhances vascularity around the wound area, the general appearance of the wound was healthier than the untreated SM wound. Aloe vera gel has also shown to be very effective in burn injuries.[28],[29] However, a clinical trial conducted to relieve the side-effects on the skin site of breast cancer patients following radiation therapy was not beneficial.[30],[31] The present study shows that percutaneously administered SM can cause oxidative stress with a decrease in GSH and GSSG concentrations and an increase in MDA content. Oral administration of Aloe vera gel protected marginally. However, dermal application of Aloe vera gel protected the skin lesions induced by SM and improved the healing process. REFERENCES
Copyright 2005 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph05019t3.jpg] [ph05019t6.jpg] [ph05019f2.jpg] [ph05019f1.jpg] [ph05019t1.jpg] [ph05019t4.jpg] [ph05019t5.jpg] [ph05019t2.jpg] [ph05019f4.jpg] [ph05019f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}