 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 37, No. 5, September-October, 2005, pp. 320-324 Research Paper "Quick Cycle" neoadjuvant chemotherapy in squamous cell carcinoma of cervix A. Taneja, S. Rajaram*, S. Agarwal**, K.C. Singh*, S. Sahni***, N. Goel Department of Obstetrics& Gynecology, Dayanand Medical College &
Hospital, Ludhiana, Punjab
*Department of Obstetrics and
Gynecology, University College of
Medical Sciences & Guru Teg Bahadur
Hospital, Delhi
** Department of Pathology, University
College of Medical Sciences & Guru Teg
Bahadur Hospital, Delhi
*** Specialty Ranbaxy, Mumbai,
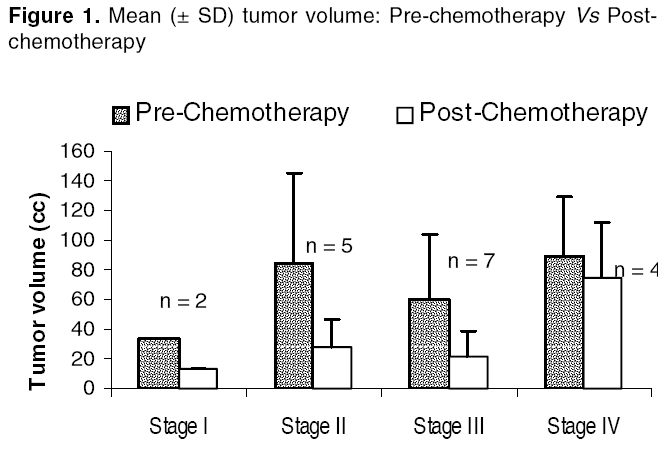
Maharashtra, India Date of Submission: 05-Apr-2004 Code Number: ph05082 Abstract Objective: To evaluate the efficacy and safety of a 'Quick cycle' neoadjuvant chemotherapeutic regime in squamous cell carcinoma (SCC) of cervix and monitor the response to chemotherapy using Squamous Cell Carcinoma Antigen (SCC-Ag) as tumor marker.Materials and Methods: Thirty patients with SCC of cervix (Stage I-IV) entered the study to receive three courses of multiagent neoadjuvant chemotherapy (vincristine, cisplatin and bleomycin) in a weekly regime. SCC-Ag was evaluated in these patients' pre and post-chemotherapy. Results: Patients with stage IB2 had a complete response and two of seven patients with stage IIB became operable. The overall response rate was 47.8% and complete response rate was 8.7%. Decrease in tumor volume post-chemotherapy was significant (P<0.002). Toxicity including myelosuppression was minimal. A statistically significant decrease in SCC-Ag (stage II and III) was seen post-chemotherapy (P <0.04 and 0.005, respectively). Conclusion: The weekly chemotherapeutic regime was found to be safe and effective and SCC-Ag is a useful tumor marker for monitoring response to chemotherapy. Keywords: Cancer cervix, SCC-Antigen, tumor marker Introduction Carcinoma cervix is the commonest malignancy in women in India yielding an incidence of 19.4 to 43.5 per 100,000.[1], [2] In India, most patients present in advanced stages and the prognosis is directly related to the stage at presentation. Five-year survival rates are 65% in stage IIB, 40% in stage IIIB, and less than 20% in stage IVA disease.[3] To date, surgery and radiotherapy have been the mainstay of the treatment for carcinoma cervix, which is curative in early stage disease, but survival considerably decreases in advanced stages.[3], [4] In an effort to improve the survival rates, neoadjuvant chemotherapy in cancer cervix has been used. [5],[6],[7]Neoadjuvant chemotherapy arrests growth and controls micro metastasis and may improve subsequent control by surgery or radiotherapy. Adjuvant chemotherapy after radiotherapy causes fibrosis and poor delivery of drug to the tumor. Traditionally chemotherapeutic regimens have been cycled 3 weekly and require at least 9 to 12 weeks before the patient can be considered for definitive therapy.[8] A ′Quick- Cycle′regime, which is cycled weekly, not only decreases the time to definitive therapy but also prevents the rapid regrowth of tumor cells.[5], [6] No study has reported the increase of the side effects with subsequent radiotherapy.[8] In the clinical setting, monitoring response to chemotherapy with tumor markers has not been universal in squamous cell carcinoma of cervix. A number of tumor markers such as CEA and TPA have been studied in cancer cervix but Squamous Cell Carcinoma Antigen (SCC-Ag) appears to be the most sensitive and specific. [9],[10],[11] In India, a waiting period of 4 to 6 weeks exists for definitive radiotherapy and this may be critical to the outcome of the disease. Therefore ′Quick Cycle′ chemotherapy, during this period may form an important adjunct without hampering conventional treatment. Thus, this study was planned to evaluate the efficacy and safety of a ′Quick-Cycle′neoadjuvant chemotherapeutic regime in squamous cell carcinoma of cervix and to monitor response to chemotherapy using SCC-Ag as a tumor marker. Materials and Methods The study was conducted in the Department of Obstetrics and Gynecology, Guru Teg Bahadur Hospital and University College of Medical Sciences, Delhi, India, over a period of 1 year (2000-2001). It was a prospective, nonrandomized study conducted in patients with stage IB2 to stage IV squamous cell carcinoma of cervix. The study was approved by the hospital ethical committee, and an informed consent was obtained from all patients. Out of the 30 patients who entered the study, 23 with proven SCC of cervix fulfilled the eligibility criteria of receiving chemotherapy, the eligibility criteria being, age less than 60 years, adequate hematological, renal and hepatic functions, no prior therapy for carcinoma cervix and histopathologic diagnosis of primary squamous cell carcinoma cervix. Locally advanced (stage IB2 and IIA) and advanced (IIB-IV) cases of carcinoma cervix received neoadjuvant chemotherapy. Patients (n=23) after completion of chemotherapy were evaluated for receiving either definitive surgery and/or radiotherapy. Patients were given three courses of multiagent neoadjuvant chemotherapy in the form of VBP regimen (vincristine 1 mg/m2 on day 1 and cisplatin 50 mg/m2 on day 1, bleomycin 15 mg/m2 on day 1 and day 2) on a weekly basis; modified regime used by Sardi et al .[5] A standard antiemetic regime consisting of metoclopramide and dexamethasone was administered. Each subsequent course of chemotherapy was administered only when the hematological, renal, and hepatic functions were within normal limits. Toxicity was evaluated by modified gynecologic oncology group (GOG) criteria. SCC-Ag was estimated by microparticle enzyme immunoassay (MEIA) with Abott IMx system using SCC-Ag and anti-SCC-Ag coated microparticles, before and after therapy in 23 patients. A value of 2.5 ng/mL or below was taken as normal. Pre-chemotherapy SCC-Ag values were further subdivided into 3 groups namely, <5 ng/mL, 5-30 ng/mL and >30 ng/mL to assess response to chemotherapy. Ohno et al in their study of prediction to radiation response used 4 groups namely, < 1.5 ng/mL, 1.5-5 ng/mL, 5-30 ng/mL and >30 ng/mL.[12] Response was assessed using standard criteria. Statistical analysis was done with paired t-test, one-way ANOVA with Tukey test, Wilcoxon Matched-Pairs Signed-Ranks test, and regression analysis. P<0.05 was considered significant. Results Patient characteristics Symptoms Tumor characteristics The mean pre-chemotherapy tumor volume for stage I was 33.95 cm3, 83.81cm3 for stage II, 59.87 cm3 for stage III, and 90.0 cm3 for stage IV. There was a statistically significant reduction in tumor volume after the completion of VBP regime and is depicted in [Figure - 1]. The reduction in volume after chemotherapy was 61.7%, 65.4%, 63.3%, and 16.6% for stage I, II, III, and IV, respectively. Mean reduction in tumor volume after therapy was 60.3%, and this was statistically significant (P <0.002). The overall response rate (sum of partial and complete response; Complete response - complete disappearance of tumor; Partial response - 50% or greater tumor volume reduction) in this study was 47.8% with a complete response rate of 8.7% and partial response of 39.1%. The response rates in various stages are shown in the [Table - 1]. Two patients with stage IB2 had complete response (complete disappearance of tumor both clinically and histopathologically at the end of treatment), and two patients of stage IIB had disappearance of parametrial growth and became operable after chemotherapy. Thus, a total of four patients out of 23 underwent radical hysterectomy after chemotherapy. Toxicity The mean value of SCC-Ag before chemotherapy in stage IB2 was 4.58 ng/mL, 13.07 ng/mL in stage II, 91.71 ng/mL in stage III, and 205.3 ng/mL in stage IV. Thus, SCC-Ag values were stage dependent. These values decreased to 0.4 ng/mL, 6.74 ng/mL, 1.89 ng/mL, and 117.9 ng/mL in stage I, II, III, and IV, respectively. The decrease after chemotherapy was statistically significant in stage II and III (P <0.04 and 0.005). There was a positive and significant correlation of tumor volume and SCC-Ag post-chemotherapy using the Wilcoxon Matched-pairs Signed-ranks test [Figure - 3]. Regression analysis showed that post-chemotherapy tumor volume (post CT-TV) significantly correlates with pre-chemotherapy volume (pre CT-TV) and SCC-Ag (P <0.001; Post CT-TV = 0.126 (SCC-Ag) + 0.22(pre CT -TV) + 9.82). Pre-chemotherapy SCC-Ag values were further subdivided into three groups namely <5 ng/mL, 5-30 ng/mL, and > 30 ng/mL. It was found that the tumor volume post- chemotherapy decreased by 58% (from 65.5 cm3 to 27.6 cm3 in group I; n=3) and by 65% in group II (from 62 cm3 to 21.4 cm3, n=13), while there was no decrease in tumor volume when SCC-Ag levels were more than 30 ng/mL (n=4)(72.4 cm3 to 72.3 cm3). The difference was statistically significant in group II (P<0.01). Discussion In this study, 91.3% of patients presented in advanced stage, namely stage IIA and above. Caplash and Sobiti reported a similar presentation in India.[13] Sixty-one percent of patients were free of the distressing symptoms of cancer cervix, namely foul smelling discharge and vaginal bleeding after therapy and this forms an important symptomatic response. The mean tumor volume was 62.64 cm3 and 80% of patients had an exophytic tumor. Tumor volume after therapy decreased to 24.85 cm3 and this decrease was statistically significant (P<0.002), thus, establishing the efficacy of the weekly VBP regime. The complete response in this study was 8.7% and partial response was 39.1%. Thus, the overall response was 47.8%. The lower response rates are probably attributed to the large number of patients presenting with advanced stage disease. Serur et al used cisplatin, vincristine, and bleomycin every 10 days for 3 cycles, and found an overall response rate of 90%.[14] However they selected patients with stage IB2 SCC of cervix and thus, had better response rates.[14] In the study by Seoud et al using the same chemotherapeutic regime similar to the present study given every ten days in advanced cervical cancer, they reported a complete response of 38% and partial response of 76%.[15] Sardi et al using vincristine, bleomycin, and cisplatin every 10 days for 3 courses found a response rate of 85% in stage IIB and 47% in stage IIIB, comparable to response rates in this study.[5] In the final report of Sardi et al , patients with stage IB2 had 83.6% of complete or partial response to chemotherapy. The overall survival after 9 years of follow-up was 61.3% for the control group (no chemotherapy) and 80% for neoadjuvant group (P <0.01). Resection was possible in 85% of control group and 100% of neoadjuvant group. Thus, neoadjuvant chemotherapy improved resectability and survival in patients with stage IB2.[6] In this study, patients with stage IB2 had a complete response of 100% [n=2] and two patients out of seven with stage IIB cancer became operable. Thus, radical surgery could be done in 44.4% of locally advanced cancers (stage IB2- IIB) or 28.5% of stage IIB cancers. In advanced stages III and IV, a partial response of only 40% was seen but there was no progression of tumor. This shows that efficacy of chemotherapy was better in early stage cancers. Palliative treatment in advanced stages using chemotherapy is of potential advantage in India where the load of carcinoma cervix is high and a long waiting period for definitive radiotherapy exists. The regime used is relatively non-myelosuppresive with no major side effects and subsequent addition of radiotherapy in these patients may improve survival with local control of disease. The mean pre-chemotherapy tumor volume of 62.64 cm3 decreased to 24.85 cm3 after therapy and this decrease was statistically significant (P <0.002). Huang et al also showed that neoadjuvant chemotherapy is effective in tumours with a tumor size of 5 cm3.[16] The current weekly chemotherapeutic schedule was found to be not only efficacious but also safe. There was no toxicity-related death. Similar results were shown by Porzio et al .[17] Toxicity-related deaths due to severe myelosuppression have been noted in other studies using adjuvant chemotherapy.[18] Hematological, renal, hepatic, pulmonary, and other toxicities were evaluated pre and post-chemotherapy. A decrease in platelet count was observed from 2.4 x 109/L to 1.6 x 109/L after therapy, which was statistically significant (P=0.00) but could not be graded as grade I toxicity of GOG criteria. Thus, the non-myelosuppressive nature of this regime makes it suitable for Indian women, majority of whom are anemic and also have intermittent, irregular, and heavy loss of blood due to the disease itself. Hepatic function remained essentially unchanged. A nonsignificant trend towards improved renal function was seen. All patients had grade II nausea and vomiting. This may be attributed to the relief of compression of ureters by the tumor due to a decrease in tumor volume. This was comparable to other studies and the need for a better antiemetic drug was felt. SCC-Ag is a relatively new, noninvasive tumor marker in carcinoma cervix. It helps not only in monitoring response to the therapy but also in detecting its early recurrence. Our study is in agreement with the previous studies showing a correlation between SCC-Ag and stage, as the plasma concentration depends on the tumor load, and SCC-Ag values increased with advancing stages.[10] The mean values of SCC-Ag in all stages (I-IV) were above the cut-off normal values of 2.5 ng/mL. SCC-Ag is a reflection of tumor bulk, intrinsic biologic tumor characteristics, and invasiveness of tumor.[19] On comparing the pre-treatment SCC-Ag values with post-treatment values, a statistically significant reduction was seen in stage II and III (P <0.04 and 0.005). The percentage reduction in stage I, II, III, and IV was 90%, 47.6%, 98%, and 42.3%, respectively. Thus, the objective of monitoring the effect of chemotherapy with the use of SCC-Ag assay is to obtain an evaluation of clinical response as early as possible and predict which of these patients will subsequently respond to surgery and/or radiotherapy. de Bruijn et al reported a decrease of SCC-Ag in 91% of cases who received chemotherapy before radiotherapy.[11] A positive and significant correlation was seen between SCC-Ag and tumor volume post- chemotherapy. Pre-chemotherapy SCC-Ag also predicts response to chemotherapy and when SCC-Ag was between 5 and 30 ng/mL a significant response to chemotherapy was seen (P < 0.14). A similar response was seen by Ohno et al when SCC-Ag was studied in relation to radiation.[12] In conclusion, the weekly neoadjuvant chemotherapy used in this short-term study was both efficacious and safe. Early-stage cancers had high response rates and a significant number became operable. No progression of disease was seen in advanced stages. This is of potential advantage in a country like India where the load of carcinoma cervix is high and a long waiting period for radiotherapy exists. Despite being cycled weekly, it was a relatively non-myelosuppressive regime. SCC-Ag is a promising new tumor marker and can be used routinely to monitor response to therapy. Acknowledgments I am thankful to Prof. D.K. Srivastava, Medical Superintendent of Guru Teg Bahadur Hospital for his unstinted help in making this study possible. References
Copyright 2005 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph05082t1.jpg] [ph05082f2.jpg] [ph05082f3.jpg] [ph05082f1.jpg] |
| |||||||||

{kind=link}
![[Table - 1]](/showimage?ph/photo/ph05082t1.jpg){kind=link}
![[Figure - 2]](/showimage?ph/photo/ph05082f2.jpg){kind=link}
![[Figure - 3]](/showimage?ph/photo/ph05082f3.jpg){kind=link}