 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
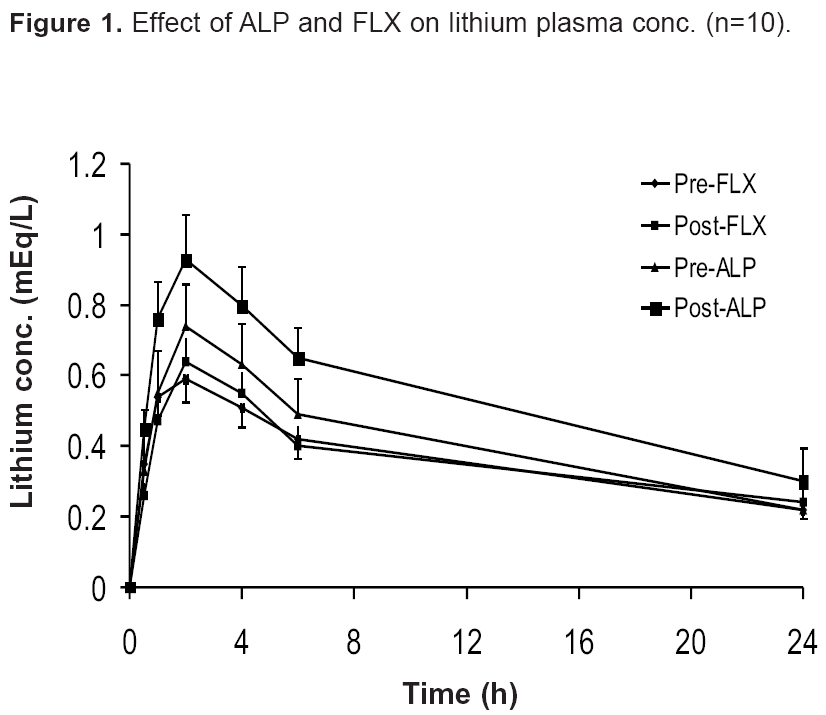
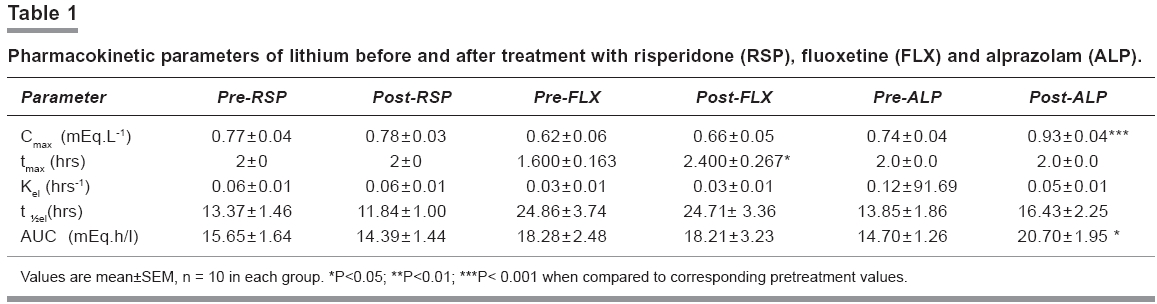
Indian Journal of Pharmacology, Vol. 38, No. 2, March-April, 2006, pp. 133-134 Research Letter Effects of fluoxetine, risperidone and alprazolam on pharmacokinetics of lithium in patients with psychiatric illnessB. Gupta*, S.C. Chopra*, C. Gupta*, R. Mahajan#, B. Uppal@ , K.B. Minocha* *Department of Pharmacology and #Psychiatry, Dayanand Medical College and Hospital, Ludhiana Code Number: ph06033 Lithium, used in manic depressive psychosis (MDP), has a narrow therapeutic index. Its effective, safe concentrations are between 0.6 and 1.25mEq/L.[1] Antidepressants[2] and neuroleptics[3] are commonly used with lithium, therefore, it is important to consider the risk of potential pharmacokinetic drug interactions among them. This study was undertaken after the Institute Ethics Committee′s approval, to examine the effects of single daily doses of risperidone (RSP), fluoxetine (FLX), and alprazolam (ALP) on pharmacokinetics of lithium in three groups of psychiatric patients. Each group had 10 patients (n = 30), and the grouping was based on patients′ psychiatric profile and treatment, as indicated. Group I. Schizophrenia or bipolar mood disorder - risperidone indicated Patients of either gender visiting the psychiatry OPD were included in the study. They were in the age group 17-55 years and were suffering from schizophrenia, endogenous depression, or chronic anxiety. These diseases were diagnosed clinically, using validated rating scales. Patients with a history of intake of drugs interacting with lithium, RSP, FLX, or ALP; significant cardiovascular, renal, hepatic, or neurological derangement; consumption of more than 30 ml of alcohol per week; and consumption of more than two cigarettes per day were excluded from the study. After an overnight fasting, a single dose of lithium 900 mg was administered orally with 200 ml of water. This was followed by a standard breakfast (Day 0). Blood samples were collected at 0, 0.5, 2, 4, 6 and 24 hours. Serum was separated and lithium levels determined by flame photometry (Systronic Mediflame 127). Appropriate drugs (risperidone 4 mg to group I, fluoxetine 20 mg to group II, and alprazolam 0.75 mg to group III) were given as a single oral dose daily at bedtime, for 14 days. In the morning of the 15th day, a single dose of lithium 900 mg was administered orally. Blood samples were collected as on day zero and lithium levels determined. Various pharmacokinetic parameters, such as, maximal plasma concentration (Cmax ), time to Cmax (tmax ), rate constant for elimination (Kel ), elimination half-life (t½e l), and area under curve (AUC) were determined by non-linear pharmacokinetic analysis. Comparisons were made between the pre- and post-drug lithium levels within each group (n=10), using paired t-test. P< 0.05 was considered significant. ALP treatment increased the plasma lithium concentrations at 0.5, 1, 2, 4 and 6 h. [Figure - 1] ALP increased both Cmax (P< 0.001) and AUC (P< 0.05) of lithium. FLX treatment [Table - 1] increased the tmax. (P< 0.05) of lithium, while there was no significant change after RSP treatment. Pre-drug lithium Cmax was lower and plasma t½ longer in all the three groups of patients in this study, compared with the untreated group in the previous study from the same laboratory.[2] The tmax was one hour in the previous study, indicating faster absorption. The slower absorption in this study appears to be due to the sample used. The previous study used several volunteers who were non-Punjabis and belonged to the lower or the middle class. This study enrolled affluent Punjabi patients who could afford treatment in a private hospital. Similarly differences in t 1/2 were reported in the Western literature also.[3] Variations in Cmax could also be due to differences in investigators and laboratory workers involved and proprietary preparations of lithium used. Plasma t½ of FLX group was longer compared with the ALP group, indicating slower elimination of lithium. Although one feels tempted to attribute this difference to a general slowing of body functions in patients with depression, there is a need for direct evidence to confirm or refute these findings. This study did not find any pharmacokinetic interaction between RSP and lithium. The increase in oral bioavailability of lithium after two weeks of ALP treatment can be explained by the fact that comorbidity of gastrointestinal symptoms and psychiatric phenomena is common. Anxiety may increase swallowing rates, exacerbating esophageal dysmotility.[4] This may have led to reduced absorption of lithium. Antianxiety treatment was expected to improve the patient symptomatically (including sympathetic over activity), resulting in normalisation of GIT motility and better absorption of drugs like lithium. Although the plasma lithium concentrations with a single dose remained within the normal therapeutic range, the Cmax increased by 25%. The physician must be aware of the possibility of lithium concentrations reaching toxic range when full therapeutic doses of lithium and ALP are co-administered. FLX reduced the absorption rate, possibly because of its slight antimuscarinic effect. This can be equated with the slow release preparations of lithium which minimise the early peaks leading to a reduction in the absorption rate. It appears that the autonomic effects of psychotropic drugs coupled with other mechanisms, may alter the bioavailability of other drugs, including lithium. Improvement in the underlying psychiatric problem can result in GIT function modulation and, therefore, bioavailability of drugs like lithium. In this study, ALP significantly increased the oral bioavailability of lithium indicating the need for extreme caution and therapeutic drug monitoring of lithium when the two drugs are combined. This study was a single dose study. Multiple dose studies are required for further confirmation of the findings and to see the changes in proper perspective. Despite this, the magnitude of change found in this study is significant. Multiple dose studies are underway and their results should provide crucial answers. To conclude, future pharmacokinetic studies of psychotropic drugs should try to correlate a quantifiable improvement in psychiatric disorders with any changes in pharmacokinetic profile of psychotropic drugs. References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06033t1.jpg] [ph06033f1.jpg] |
| |||||||||

{kind=link}
{kind=link}