 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 38, No. 3, May-June, 2006, pp. 171-176 Education Forum Orphan diseases and drugs Randhawa GK Department of Pharmacology,Government Medical College, Amritsar, Punjab Code Number: ph06042 Abstract The World Health Organization defines orphan diseases, as all pathological conditions, affecting 0.65-1 out of every 1000 inhabitants. They are usually not studied for their pathophysiology or for newer therapeutic options, as these are not economically viable. The Orphan Drug Act was passed on January 28, 1983 by USA to stimulate the research, development and approval of those products that treat orphan diseases. Till date, 11 drugs (4.87%) for tropical infectious diseases have been designated with orphan drug status and as many drugs for other infectious diseases. Several drugs with orphan status are used in the treatment of diseases that no longer meet orphan status criteria, such as AIDS and end-stage renal disease. Understanding of the human genome, nuclear cloning, rational drug designing and application of high throughput screening in drug discovery programs, might lead to new drug discoveries for orphan diseases. Hence, there is hope in future for patients neglected by for-profit drug discovery efforts.Keywords: Drugs for neglected diseases initiative, neglected diseases orphan drugs. The World Health Organization defines orphan/rare diseases as, 'all pathological conditions that affect 0.65-1 out of every 1000 inhabitants'. The EU defines a rare disorder as one with a prevalence of 5: 10,000 Europeans; the USA accepts it as an ailment affecting fewer than 2,00,000 Americans (with an incidence of less than 1/5,000 in the general population); Japan has the limit at 50,000 Japanese patients and Australia at 2000 Australian patients.[1] There are approximately 6,000 orphan diseases, out of which 80% are genetic.[2] These diseases are very much like children without parents and as such, require special effort for the development of their treatment options. But they are usually not studied for their pathophysiology or for newer therapeutic options,[3] as the inputs are not economically rewarding. Hence, treatment and diagnostic methods also have not yet been fully developed for them. Many orphan diseases are lesser known, like Juberg Marsidi syndrome (a genetic disorder of childhood that leads to severe mental retardation, abnormal bone growth resulting in the disfiguring of the head and body and loss of hearing), Hermansky-Pudlak syndrome (a group of genetically heterogeneous disorders which share the clinical findings of oculocutaneous albinism, platelet storage pool deficiency and ceroid lipofuscinosis), Werdnig Hoffman disease (a fatal, fetal disease similar to amyotrophic lateral sclerosis (ALS), Omenn's syndrome (absence of mature B and T cells, children being born with late-stage ALS-like symptoms), Fabry's disease (an X-linked lysosomal-storage disorder due to deficiency of galactosidase A), Lambert-Eaton myasthenic syndrome (an autoimmune disease of peripheral cholinergic system resulting in muscle weakness due to impaired acetylcholine release) and many more like Aarskog syndrome, Adams Nance syndrome, Bagatelle Cassidy syndrome, Bamforth syndrome, Ballard syndrome and Bahemuka Brown syndrome . There are some familiar orphan/rare/neglected diseases, like Alzheimer's disease, ALS , Crohn's disease, Hodgkin's disease, leukemia ( many forms ), multiple sclerosis, Huntington's disease, sickle cell disease, muscular dystrophy, myasthenia gravis and spinal cord injury . All disorders due to genetic defects in development (like spina bifida, Turner's syndrome, Klinefelter's syndrome, cleft lip and palate ) and deficient enzymes (like cystic fibrosis, respiratory distress syndrome, Gaucher's disease, hemophilia ), are considered orphan diseases. Tropical infectious diseases like malaria, leprosy, tuberculosis and leishmaniasis with lesser incidence in developed countries, may also be considered as orphan diseases there. Concept of orphan drug Medical melodrama in the early 1980's in the US, set the pace for the concept of orphan drug and its regulation. It depicted a young boy with Tourette syndrome, which generated the public opinion for unfortunate victims of these diseases. With this issue in the public eye, the Orphan Drug Bill was passed in 1981, but the US Congress stalled it.[4] A specific treatment of the orphan condition was not lucrative for the pharmaceutical industry, as these medicines would be used only by a small number of patients. There is a 13-fold greater chance of a medicine being brought to market for central nervous system disorder or cancer, than for a neglected disease.[5] There was no incentive for the pharmaceutical industry to spend time (around 10 years) and money (the cost of bringing a new molecules approximately $350-500 million) on unproductive ventures.[6] Moreover, research had to be prioritized to make best use of available resources. This gave rise to the concept of orphan drugs which lack sponsorship, are expensive to investigate and develop, are used by few patients and bring inadequate rewards Therefore there is very little incentive for marketing these.[7]Need for orphan drug regulation Absence of specific treatment for orphan disease causes psychological distress to the patient and the family and a feeling of hopelessness sets in. Many diseases lacking specific therapy are important targets for anecdotal therapy. Thus, unproven therapies and wrong beliefs prevail in quest of some relief. USA was the first nation to propose a legal framework to encourage development and availability of orphan drugs.[8],[9] The Orphan Drug Act (ODA) was passed on January 28, 1983, which was an amendment of Federal Food, Drug and Cosmetic Act of 1938,[10] to stimulate the research, development and approval of products that treat orphan diseases. Drugs are granted orphan status for a specific indication and still need studies to demonstrate their safety and efficacy, unless these qualify for accelerated approval. The main incentives of achieving orphan drug status (ODS) include:
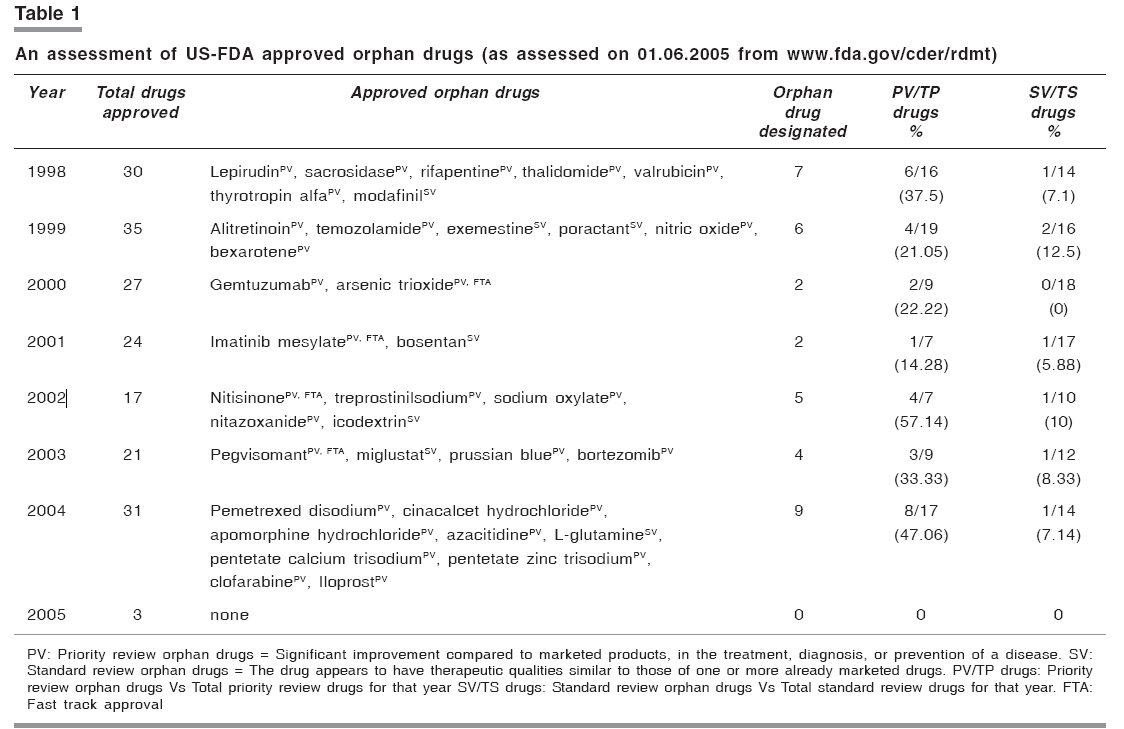
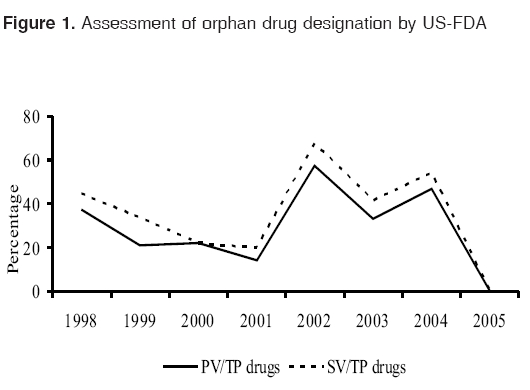
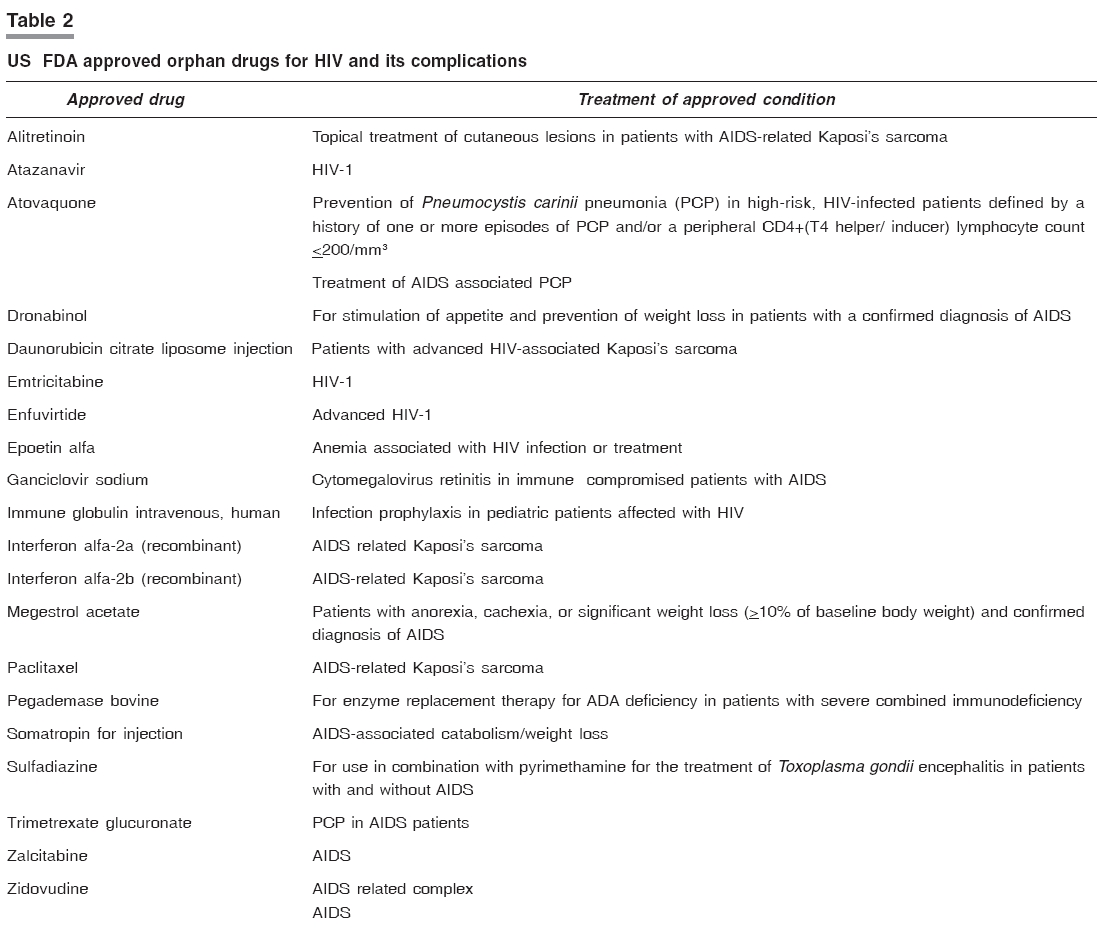
More than 10 million patients have been treated since the inception of ODA, which has fueled research of orphan diseases. ODA exists in various countries like USA, Japan, Singapore, Australia, Canada, France, Sweden and United Kingdom.[12] The basis of the initiative of other countries being the US ODA, with variations like marketing exclusivity rights to the marketing company for 7 years in USA, 10 years in Japan and 5 years in Australia. Other countries seeking to establish similar legislation include South Korea, New Zealand and India. A group of pharmacologists requested the Indian government to institute ODA at the conference held by the Indian Drug Manufacturing Association in November 2001,[13] but nothing concrete has materialized so far. Fast-track drug designation After the thalidomide tragedy, it was realized that more rigorous phase II and III clinical trials, were required prior to approval for marketing of a drug. But in recent times, the situation has changed. The AIDS crisis has prompted a swing back from the expensive and rigorous pre-marketing review, to more expedited/fast track processes, with the intention of getting relief from fast spreading and fatal diseases.[14] Fast-track designation does not apply to a drug alone, but to the combination of a drug and the specific indication being studied. Drugs intended to treat a serious condition must be therapeutic (treat a serious manifestation or symptom), diagnostic (improve detection or diagnosis), preventive (prevent serious consequences) or lack serious adverse effects. For fast-track designation, one of the two conditions must be met: (1) no therapy must exist for that specific condition, (2) the new therapy must demonstrate an improved effect, affect alternative outcomes other than the current therapy, benefit patients unresponsive to current therapy, avoid serious toxicities associated with current therapy or offer improved compliance and convenience compared to current therapy.[15] Postmarketing surveillance for these drugs present concern because of small number of target patients. Potential issues may include drugs approved for orphan status for diseases that no longer are considered rare (like AIDS) or drug approval based on surrogate endpoints that later do not demonstrate a traditional benefit. [Table - 1] FDA approvals for ODS are less, as compared with total approval of new molecular entities. As can be seen from the above data, that percentage of orphan drugs for standard approvals is much less (0% in 2000 to 7.14% in 2004), as compared to priority approvals (22.22% in 2000 to 47.26% in 2004). In 2005, no drug was approved for ODS. Except for 2002, it is clear that the interest of pharmaceuticals for development and subsequent approvals for ODS is lacking. [Figure - 1] Fast track approval has been granted to four drugs during these eight years for various conditions: Arsenic trioxide was approved on 25.09.2000 for treatment of acute promyelocytic leukemia, Imatinib mesylate on 10.05.2001 for chronic myeloid leukemia, nitisinone on 18.01.2002 for hereditary tyrosinemia type-I and pegvisomant on 25.03.2003 for acromegaly. With the advent of ODA, considerable drugs (16.55%) are being developed for orphan diseases. Approval for ODS by FDA has been given to 269 drugs (as on 15.05.2005). Some of the agents approved for genetic/congenital diseases as replacement therapy, are recombinant enzyme imiglucerase and alglucerase (injection) in patients with gaucher's disease, antithrombin III (human) for congenital deficiency of AT-III, for prevention and treatment of thrombosis and pulmonary emboli, alpha-1 proteinase inhibitor (human) for alpha-1 proteinase inhibitor congenital deficiency state, coagulation factor IX (human) for patients with hemophilia B for the prevention and control of bleeding episodes and during surgery to correct defective hemostasis, pegademase bovine for ADA deficiency in patients with severe combined immunodeficiency, somatropin for growth hormone deficiency in adults after epiphyseal closure. Approved agents for treatment of some of the genetic diseases are felbamate , topiramate and lamotrigine for Lennox-Gastaut syndrome, levocarnitine for carnitine deficiency, octreotide for acromegaly, riluzole for ALS, sacrosidase for sucrase-isomaltase deficiency, tranexamic acid for coagulopathies receiving surgical intervention (e.g. dental extractions). Very few new medicines are being developed for orphan diseases. Current options for Wilson's disease with neurologic manifestations, are anticopper drug-penicillamine (which often makes the patient neurologically worse) and zinc (which is slow acting) with many adverse effects. A newly developed (2003) orphan drug ammonium tetrathiomolybdate acts differently from previous anticopper medicines. It forms a stable tripartite complex with copper and protein. An open-label study of this (120 to 410 mg/day, for eight weeks with maintenance therapy with zinc for 3 years) in 55 untreated, newly diagnosed patients with neurological manifestations, reported that it is highly effective in them.[16] About 2.7% of all the new medicines (1061) developed from 1975 to 1994, concerned tropical diseases. A few novel medicines have been developed from veterinary medicine ( ivermectin ) and military research, (halofantrine, mefloquine) as orphan drugs. Analysis of pharmacopoeia resulted in the development of artesunate, artemether and arteether . Lesser importance is being given to the development of newer treatment options for tropical infectious diseases, which is of concern to nations with endemicity of these diseases. Combined effect of minimal development of pharmaceutical agents, development of chemoresistance to older medicines ( chloroquine, sulfadoxine-pyrimethamine, aminopenicillins ), affordability (second and subsequent generation molecules) and the abandonment of major medicines ( melarsoprol ) pose hurdles in treatment of these diseases.[17] Our net search revealed that, 11 drugs (4.87%) for tropical infectious diseases have been designated with ODS and as many medicines for other infectious diseases. US FDA has approved various orphan drugs for tropical infectious diseases, whose incidence is less in developed countries, but common in tropical countries. Halofantrine and mefloquine have been approved as antimalarials, whereas rifabutin, rifampin, rifapentine, isoniazid, pyrazinamide and aminosalicylic acid have been approved as antitubercular agents. Thalidomide and clofazimine have been approved as antileprosy, liposomal amphotericin B for visceral leishmaniasis and eflornithine for sleeping sickness. US FDA has approved albendazole as orphan drug for neurocysticercosis due to Taenia solium as: 1) chemotherapy of parenchymal, subarachnoidal and racemose (cysts in spinal fluid) neurocysticercosis in symptomatic cases and 2) prophylaxis of epilepsy and other sequelae in asymptomatic neurocysticercosis and hydatid disease (cystic echinococcosis due to E. granulosus larvae or alveolar echinococcosis due to E. multilocularis larvae), amphotericin B lipid complex for invasive fungal infections, cromolyn sodium 4% ophthalmic solution for vernal keratoconjunctivitis, daptomycin for complicated skin infections, efalizumab for moderate to severe psoriasis, ganciclovir intravitreal implant for cytomegalovirus retinitis, gemifloxacin for acute exacerbation of bronchitis and community acquired pneumonia. Others having been granted ODS are liposomal amphotericin B for cryptococcal meningitis, lodoxamide tromethamine for vernal keratoconjunctivitis, pentamidine isethionate for Pneumocystis carinii pneumonia, prevention of Pneumocystis carinii pneumonia in patients at high risk of developing this disease, respiratory syncytial virus immune globulin (Human) for prophylaxis of respiratory infections in infants and young children, at high risk. The other drugs with ODS are mafenide acetate solution for use as an adjunctive topical antimicrobial agent, when used under moist dressings over meshed autografts on excised burn wounds, ofloxacin for bacterial corneal ulcers, sertaconazole for athletes foot and tobramycin inhalation for bronchopulmonary infection of Pseudomonas aeruginosa in cystic fibrosis. Hazards of orphan drugs Orphan drugs may be associated with greater hazard than other products, as ideal amount of clinical evidence is often lacking. [18] For example, during clinical testing, 31% of orphan drugs on the market had more pronounced adverse effects than non-orphan medicinal products. Similarly after FDA approval, 13% of orphan products provoked more side effects than anticipated.[19]Orphan vaccines In addition to orphan drugs, there are orphan vaccines for disease control and the prevention of spread of contagious diseases. Vaccines are expensive to develop for a small number of rare infectious diseases and for those important but geographically limited diseases (such as arboviral or diarrheal), involving a small number of people. Only eight vaccines registered with orphan status (seven for therapeutic indications e.g., cancer and sickle cell anemia and one to prevent an Asiatic infectious disease - Japanese encephalitis virus), have been developed.[20] Effective vaccine against common infectious diseases like malaria, tuberculosis and dengue fever, being still not available, tropical countries will have to find a way to develop their own vaccine facilities, [21] from a centralized non-profit public enterprise.Devices with ODS Devices intended to benefit the patient by treating or diagnosing a disease or condition that affects or is manifested in fewer than 4,000 individuals in the US per year, paved the way for Humanitarian Use Devices through The Safe Medical Devices Act of 1990.[22] Some of these are, thyrotropin alpha as an adjunct to diagnosis of thyroid cancer, synthetic porcine secretin for use in diagnosis of gastrinoma associated Zollinger-Ellison syndrome, satumomab pendetide for detection of ovarian carcinoma, pentastarch as an adjunct in leukapheresis to improve the harvesting and to increase the yield of leukocytes by centrifugal measures and iobenguane sulfate I 131 for use as a diagnostic adjunct in patients with pheochromocytoma. Nuclear medicine scientists can take advantage of this Act to develop orphan radiopharmaceuticals for the treatment or diagnosis of rare diseases or conditions.ODS with non-orphan disease states Several medicines with ODS, treat diseases that no longer meet orphan status criteria, such as AIDS and end-stage renal disease.[23] Calcium acetate for hyperphosphatemia and epoetin alfa for anemia associated with end stage renal disease, were granted ODS on 10.12.1990 and 01.06.1989, respectively. Though AIDS is no longer an orphan disease, yet 20 medicines continue to have ODS. [Table - 2] Pharmaceutical companies may reap the benefits of an ODS for unlabeled use. Imatinib nonselectively inhibits the production of the Philadelphia chromosome, the stem-cell factor and events and other platelet-derived growth factor receptors.[24],[25] More than one site of action for a medicine can lead to multitude of studies, investigating its efficacy in other unlabeled uses, such as the treatment of acute lymphoblastic leukemia, thyroid cancer, glioblastoma and small-cell lung cancer.[26],[27],[28],[29] Therefore, if a medicine is efficacious in the treatment of other diseases (which increases its use beyond 2,00,000 patients), it provides substantial market advantage over medicines that are approved in a traditional manner. Most companies think of additional patient populations to study the medicine at the time of NDA submission, regardless of ODS.[30] The public -private partnerships for R & D initiatives for rare diseases, offers a new and effective way to deal with the medical needs of orphan disease patients. It can comprise of health and research institutes of different countries, along with medical organizations like World Bank, WHO, UNDP. One such initiative focusing on drugs for rare diseases is DNDi (Drugs for Neglected Diseases Initiative).[31] Future prospects It is anticipated that pharmacogenomics will result in the identification of more orphan diseases in future. Animal experimentation has shown that nuclear cloning and gene and cell therapy, represent exciting new strategies for treating genetic diseases. Nuclear transfer of embryonic stem cells (derived from mouse cumulus or fibroblast cells) can be coaxed into becoming somatic cells like myogenic cells, dopaminergic and serotonergic neurons, hematopoietic cells or pancreatic islet like cells. Strategies like therapeutic cloning might prove to be the future of treatment of neurodegenerative diseases and blood dyscrasias.[32] Adult stem cells could help to cure some rare diseases. Ethical considerations impede the development of therapeutic cloning. [33] As new technologies of drug designing are incorporated in drug discovery programs, application of these in orphan diseases might lead to better results in a shorter span of time. International support for rare disease research is also providing stimulus and motivation, to overcome the financial barriers and encourage development of treatment, for rare diseases throughout the world.[11] FDA also has come up to expedite the availability of medications needed for its own public. Hence, the future holds hope for patients who have been so far neglected due to profit oriented drug discovery efforts. References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06042t1.jpg] [ph06042t2.jpg] [ph06042f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}