
|
Indian Journal of Pharmacology
Medknow Publications on behalf of Indian Pharmacological Society
ISSN: 0253-7613 EISSN: 1998-3751
Vol. 38, Num. 4, 2006, pp. 238-242
|
Indian Journal of Pharmacology, Vol. 38, No. 4, July-August, 2006, pp. 238-242
Educational Forum
Drugs and non-alcoholic steatohepatitis
Das SK, Vasudevan DM
Department of Biochemistry, Amrita Institute of Medical Sciences, Elamakkara P.O., Cochin-682 026, Kerala
Correspondence Address:Department of Biochemistry, Amrita Institute
of Medical Sciences, Elamakkara P.O., Cochin-682 026, Kerala, subirkumardas@aims.amrita.edu
Code Number: ph06066
Abstract
Health complications associated with obesity include diabetes, hypertension, hyperlipidemia, cardiovascular disease, and associated co-morbidities including non-alcoholic steatohepatitis (NASH). Additionally, NASH has been associated with several drugs. Though steatohepatitis is a rare form of drug induced liver disease, it has generated great interest in the recent past. Oral hypoglycemic agents, lipid lowering agents, antihypertensives, and antiobesity medication underlie a significant proportion of well-recognized hepatotoxicity. While some medications have predictable toxicity, many more are associated with idiosyncratic reactions. The toxic mechanism appears to involve mitochondrial injury, impaired β-oxidation, generation of reactive oxygen species and ATP depletion. If a drug is suspected, it is probably prudent to stop this medication.
Keywords: Antihypertensive drugs, antiobesity drugs, liver disease.
Introduction
Ludwig introduced the term nonalcoholic steatohepatitis (NASH) to describe a form of liver disease that is histologically indistinguishable from alcoholic hepatitis but occurs in people who do not consume excess ethanol.[1] It is now clear that the spectrum of nonalcoholic fatty liver (NAFL) extends from non-progressive disease, through NASH and finally to "cryptogenic" cirrhosis in which steatosis may be inconspicuous.[2],[3] NASH is now conceptualized as encompassing at least three components among the tetrad of steatosis, hepatocellular injury, focal mixed cell-type inflammation and fibrosis.[4] However, there is not yet complete agreement on the semantics (NAFL versus NASH) or definition of what constitutes steatohepatitis. Pathological definition of NASH requires steatosis, significant hepatocellular injury (most often indicated by ballooning degeneration), diffuse mixed lobular inflammation, and perisinusoidal and perivenular fibrosis.[5] Drug induced steatohepatitis Drug-induced liver diseases (DILDs) are clinicopathologic patterns of liver injury related to drugs.[6] Steatohepatitis is a rare form of DILD[5],[6] and drugs account for fewer than 2% cases of NASH. It is noteworthy that drugs that cause steatohepatitis are often associated with other types of liver injury, particularly acute hepatitis. Some agents implicated as causing cirrhosis or other forms of NAFL in obese middle-aged diabetic women (methyl dopa, calcium channel blockers, estrogens, methotrexate) may be fortuitous co-associations with "primary" NASH, which most often occurs among persons with the insulin resistance or metabolic syndrome.[3],[4],[7],[8],[9] Obesity and steatohepatitis Obesity, an ever-expanding global health problem contributes significantly to individual poor health and societal burden of disease.[10] It leads to the development of more than 50 distinct medical disorders and alters the response to the treatment of many others. They include diabetes, hypertension, hyperlipidemia, and cardiovascular disease with all their associated co-morbidities. It is not surprising therefore that both the complications of obesity and, increasingly, obesity itself are aggressively targeted for pharmacotherapy. This has included oral hypoglycemic agents, lipid lowering agents, antihypertensives and antiobesity medications. These four categories of medication constitute a significant proportion of well-recognized hepatotoxic medications. In many instances, these medications have been withheld from patients because of liver abnormalities.[11] NASH is a liver disease in which obesity and insulin resistance are frequently implicated.[12] Pathology of drug induced steatohepatitis
Approximately 900 medications have been identified as potentially hepatotoxic, many of them have interactions and cross-reactivity, and the severity of injury can range from asymptomatic or mild to fatal. Medication induced hepatotoxicity can be divided into the unexpected, idiosyncratic reaction, and the predictable, intrinsically toxic one.[13] Generally, intrinsically toxic medications are not used clinically if liver function is known to be compromised. This type of liver injury is usually avoidable. However, idiosyncratic drug reactions are often not identified. The cause of these reactions is unclear and is postulated to be due to hypersensitivity, toxic metabolite production, or deficiencies of detoxification. Hypersensitivity reactions are characterized clinically by fever, rash, eosinophilia, eosinophilic infiltrates, and/ or granulomata, and tend to occur in close temporal relation to the administration of the drug. [13] Liver injury may be primarily hepatocellular, cholestatic, or mixed.
In general, drug-induced steatohepatitis resembles alcoholic liver
disease more closely than NASH associated with diabetes and insulin resistance
syndrome. Thus, cirrhosis and hepatic failure are common, and the liver
pathology shows impressive polymorphonuclear leukocyte (polymorph) inflammation,
ballooning degeneration of hepatocytes, and Mallory bodies. Progression
of fibrosis to cirrhosis can occur over weeks or months in drug induced
steatohepatitis, whereas it may take decades and often never occurs in
patients with NASH.[5]
Myeloid bodies are a characteristic ultrastructure feature of drug-induced
steatohepatitis. They are ascribed to phospholipidosis, which is a
dose dependent phenomenon attributable to the physicochemical properties
of cationic amphiphilic drugs.[14] These
properties favor accumulation of the drug in the lipid membranes and
proton-rich organelles, including lysosomes and mitochondria. Drugs
associated with phospholipidosis may inhibit lysosomal phospholipases
directly or by binding to phospholipids, thereby inhibiting the turnover
of lipid bilayers.[15] While
liver enzymes (transaminases and alkaline phosphatase) usually normalize
after withdrawal of the drug, there has been some concerns sparked
by persistent liver injury and cirrhosis following discontinuation
of drug.[16],[17],[18]
Hepatotxicity of drugs
Currently available medications in the treatment of obesity can be divided into those that decrease appetite or increase satiety. [Table - 1]
Type 2 diabetes is a well-recognized complication of obesity. It is associated with liver disease in and of itself, with the predominant etiology being NASH. Conversely, liver disease has not been associated with type 1 diabetes mellitus, which reflects the current understanding that insulin resistance, not insufficiency, is associated with this type of liver disease.[8],[26] However, it may be difficult to differentiate hepatic injury related to diabetic medications from that related to diabetes itself.
Other than insulin, the incidence of reported toxicity for sulfonylurea
is ~1%, and is felt to be caused by hypersensitivity to the sulfur
moiety.[27] Metformin, the
only biguanide currently used in the treatment of type 2 diabetes, is generally
considered to be safe, but has also shown cholestatic hepatitis.[35] The
glucosidase inhibitors are useful adjunctive therapies for Type 2 diabetes.
The prototype of this class is acarbose for which there is also a report
of hepatotoxicity.[43] The
thiazolidinediones (troglitazone, pioglitazone, and rosiglitazone) are
peroxisome proliferator-activated receptor gamma (PPARγ) ligands. They
are used in the treatment of type 2 diabetes as insulin sensitizing medications,
but their interest extends to the treat-ment of primary liver diseases,
such as steatohepatitis.[38],[44] They
have been shown to inhibit collagen deposition in animal models of fibrosis.[45]
Among the lipid lowering agents in use today, the HMGCoA reductase inhibitors
(statins) have gained notoriety for their propensity to cause transaminase
elevations. Hepatotoxicity appears to be a risk of all lipid lowering-agents.
However, the overall incidence of significant hepatotoxicity with lipid-lowering
agents is low, and concern over liver enzyme abnormalities may lead to
inappropriate withdrawal in many individuals who need therapy.[11]
There are some well known hepatotoxicity patterns associated with antihypertensive
medications. Such an example is a-methyldopa associated autoimmune hepatitis.[46] With
the advent of newer classes of antihypertensives, a-methyldopa use has
decreased. However, considering that it is one of the few antihypertensive
safe to use in pregnancy, it is still commonly prescribed in such cases.[47] Beta-blockers
are in common use, and generally have a low incidence of hepatotoxicity,
with the possible exception of labetalol. Calcium channel blockers have
been implicated in drug-induced steatohepatitis.[48]
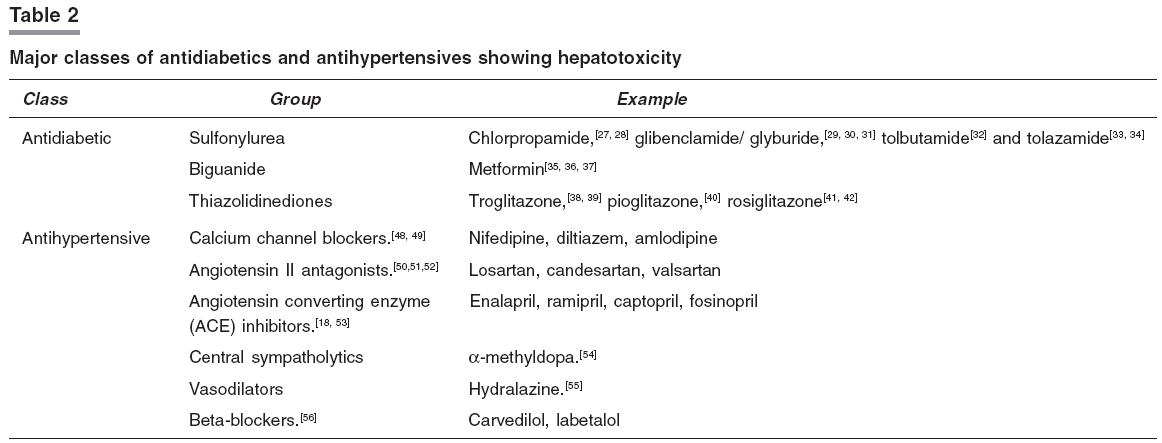
[Table - 2] summarizes
the major classes of antidiabetics and antihypertensives reported to be
hepatotoxic.
Mechanisms
There are several reasons for associations between drugs and steatohepatitis. The first possibility is that a person with NASH happens to be taking the drug for conditions associated with the insulin resistance syndrome, such as hypertension or other cardiovascular disorders. The second is that the drug may precipitate or accentuate risk factors for NASH, such as central obesity, diabetes, and hypertriglyceridemia. A third is that occult alcoholism may be involved. This has been suspected in some reported associations between industrial solvents and hepatotoxicity.[6] The final possibility is that some drugs may actually cause steatohepatitis by a direct hepatotoxic mechanism. [Table - 3] Establishing the diagnosis of drug-induced liver disease may be difficult. It requires:
(a) absence of other causes of liver disease, and
(b) that the ingestion of drug precedes the onset of liver disease.[66]
This seems to be the case for perhexiline maleate, coralgil (4, 4'-diethylaminoethoxyhexestrol),
amiodarone, and possibly for tamoxifen.[67] Perhexiline,
amiodarone, and tamoxifen can accumulate in the mitochondria and inhibit
mitochondrial β-oxidation, thereby causing steatosis.[68],[69] They
also inhibit oxidative phosphorylation. [68],[69] In
the longer-term, electron leakage with production of reactive oxygen species
(ROS), increase in lipid peroxidation and decrease in cellular ATP levels
could be of relevance to the pathogenesis of liver injury. Thus drug-induced
steatohepatitis may be a paradigm for injurious events in common metabolic
forms of NASH.[8], [9], [70], [71]
Other studies implicate peroxisome proliferator-activated receptors (PPARs)
leading to NASH.[72] PPARα
is a transcription factor that governs both microsomal ( via CYP4A)
and peroxisomal (β-oxidation) pathways of lipid oxidation and ultimately
production of ROS.[73] PPARγ
also plays a regulatory role in lipid homeostasis and is up-regulated in
livers of obese and diabetic mice.[73] Thiazolidinediones
(troglitazone, rosiglitazone), which reverse insulin resistance and correct
hyperglycemia and hyperlipemia in type 2 diabetes, also bind to and activate
this receptor.[73] It is therefore
possible that type 2 diabetes may sensitize the liver to PPARγ-activating
drugs.
Prevention Liver enzyme abnormalities and liver disease may be attributable to drugs. If a drug is suspected, it is important to determine the dose, route, and duration of therapy, as well as possible interactions.[74] The latency between drug ingestion and the appearance of disease is also important. Other causes of liver diseases must be excluded. Finally, if suspicion of drug-related injury still remains, the drug should be discontinued.
Conclusion
In addition to the usual associations with insulin resistance, type 2 diabetes,
central obesity, and hypertriglyceridemia, nonalcoholic steatohepatitis
has been associated with several drugs. Though, drug induced liver disease
is a relatively uncommon cause of steatohepatitis, it has become the single
major cause for regulatory actions concerning drugs, specifically during
drug development. In spite of the recent increased interest, very little
progress has been made toward understanding mechanisms underlying hepatotoxicity.
Early recognition of hepatotoxicity is crucial to prevent the development
of severe form of liver disease and improve the clinical outcome.
References
| 1. | Ludwig J, McGill DB, Lindor KD. Review: nonalcoholic steatohepatitis.J Gastroenterol Hepatol 1997;12:398-403. Back to cited text no. 1 [PUBMED] |
| 2. | Ratziu V, Giral P, Charlotte F, Bruckert E, Thibault V, Theodorou I, et al . Liver fibrosis in overweight patients. Gastroenterol 2000;118:1117-23. Back to cited text no. 2 |
| 3. | Marceau P, Biron S, Hould FS, Marceau S, Simard S, Thung SN, et al . Liver pathology and the metabolic syndrome X in severe obesity. J Clin Endocrinol Metab 1999; 84:1513-7. Back to cited text no. 3 |
| 4. | Brunt EM. Nonalcoholic steatohepatitis: Definition and pathology.Semin Liver Dis 2001;21:3-16. Back to cited text no. 4 |
| 5. | Farrell GC. Drugs and non-alcoholic steatohepatitis. In: Leuschner U, James O, Dancygier H, editors. Falk Symposium 121- Steatohepatitis (NASH and ASH). Dordrecht: Kluwer Academic Publishers; 2000. Back to cited text no. 5 |
| 6. | Farrell GC. Drug induced liver disease. Edinburgh: Churchill Livingstone, 1994. Back to cited text no. 6 |
| 7. | Chitturi S, Abeygunasekera S, Farrell GC, Holmes-Walker J, Hui JM, Fung C, et al . NASH and insulin resistance: Insulin hypersecretion and specific association with the insulin resistance syndrome. Hepatol. 2002;35:373-9. Back to cited text no. 7 |
| 8. | Sanyal AJ, Campbell-Sargent C, Mirshahi F, Rizzo WB, Contos MJ, Sterling RK, et al . Nonalcoholic steatohepatitis: association of insulin resistance and mitochondrial abnormalities. Gastroenterol 2001;120:1183-92. Back to cited text no. 8 |
| 9. | Angulo P, Lindor KD. Insulin resistance and mitochondrial abnormalities in NASH: A cool look into a burning issue. Gastroenterol 2001;120:1281-5. Back to cited text no. 9 [PUBMED] [FULLTEXT] |
| 10. | Kuczmarski RJ. Prevalence of overweight and weight gain in the United States. Am J Clin Nutr 1992;55:495-502. Back to cited text no. 10 [PUBMED] |
| 11. | Ghali P, Lindor KD. Hepatotoxicity of drugs used for treatment of obesity and its comorbidities. Semin Liv Dis 2004;24:389-97. Back to cited text no. 11 [PUBMED] [FULLTEXT] |
| 12. | James OF, Day CP. Non-alcoholic steatohepatitis (NASH): A disease of emerging identity and importance. J Hepatol 1998;29:495-501. Back to cited text no. 12 [PUBMED] [FULLTEXT] |
| 13. | Zimmerman HJ. Drug-induced liver disease. Clin Liver Dis 2000;4:73-96. Back to cited text no. 13 [PUBMED] |
| 14. | Pirovino M, Muller O, Zysset T, Honegger U. Amiodarone-induced hepatic phospholipidosis: correlation of morphological and biochemical findings in an animal model. Hepatol 1988;8:591-8. Back to cited text no. 14 |
| 15. | Lullmann H, Lullmann-Rauch R, Wassermann O. Drug-induced phospholipidoses II. Tissue distribution of the amphiphilic drug chlorphentermine. CRC Crit Rev Toxicol 1975;4:185-218. Back to cited text no. 15 [PUBMED] |
| 16. | Droste HT, de Vries RA. Chronic hepatitis caused by lisinopril. Neth J Med 1995;46:95-8. Back to cited text no. 16 [PUBMED] [FULLTEXT] |
| 17. | Jeserich M, Ihling C, Allgaier HP, Berg PA, Heilmann C. Acute liver failure due to enalapril. Herz 2000;25:689-93. Back to cited text no. 17 [PUBMED] |
| 18. | Yeung E, Wong FS, Wanless IR, Shiota K, Guindi M, Joshi S, et al . Ramipril-associated hepatotoxicity. Arch Pathol Lab Med 2003;127:1493-7. Back to cited text no. 18 |
| 19. | Golik A, Rubio A, Weintraub M, Byrne L. Elevated serum liver enzymes in obesity: a dilemma during clinical trials. Int J Obes 1991;15:797-801. Back to cited text no. 19 [PUBMED] |
| 20. | Weintraub M, Rubio A, Golik A, Byrne L, Scheinbaum ML. Sibutramine in weight control: a dose-ranging, efficacy study. Clin Pharmacol Ther 1991;50:330-7. Back to cited text no. 20 [PUBMED] |
| 21. | Montero JL, Muntane J, Fraga E, Delgado M, Costan G, Serrano M, et al . Orlistat associated subacute hepatic failure . J Hepatol 2001;34:173. Back to cited text no. 21 |
| 22. | Mehta H, Murray B, LoIudice TA. Hepatic dysfunction due to intravenous abuse of methylphenidate hydrochloride. J Clin Gastroenterol 1984;6:149-51. Back to cited text no. 22 [PUBMED] |
| 23. | Cai Q, Benson MA, Talbot TJ, Devadas G, Swanson HJ, Olson JL, et al . Acute hepatitis due to fluoxetine therapy. Mayo Clin Proc 1999;74:692-4. Back to cited text no. 23 |
| 24. | Friedenberg FK, Rothstein KD. Hepatitis secondary to fluoxetine treatment. Am J Psychiatry 1996;153:580. Back to cited text no. 24 [PUBMED] |
| 25. | Wernicke JF. The side effect profile and safety of fluoxetine. J Clin Psychiatry 1985;46:59-67. Back to cited text no. 25 [PUBMED] |
| 26. | Marchesini G, Bugianesi E, Forlani G, Cerrelli F, Lenzi M, Manini R, et al . Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatol 2003;37:917-23. Back to cited text no. 26 |
| 27. | Schneider HL, Hornbach KD, Kniaz JL, Efrusy ME. Chlorpropamide hepatotoxicity: report of a case and review of the literature. Am J Gastroenterol 1984; 79:721-4. Back to cited text no. 27 [PUBMED] |
| 28. | Rigberg LA, Robinson MJ, Espiritu CR. Chlorpropamide-induced granulomas. A probable hypersensitivity reaction in liver and bone marrow. J Am Med Assoc 1976;235:409-10. Back to cited text no. 28 [PUBMED] |
| 29. | van Basten JP, van Hoek B, Zeijen R, Stockbrugger R. Glyburide-induced cholestatic hepatitis and liver failure. Case-report and review of the literature. Neth J Med 1992;40:305-7. Back to cited text no. 29 [PUBMED] |
| 30. | Petrogiannopoulos C, Zacharof A. Glibenclamide and liver disease. Diabetes Care 1997;20:1215. Back to cited text no. 30 [PUBMED] |
| 31. | Saw D, Pitman E, Maung M, Savasatit P, Wasserman D, Yeung CK. Granulomatous hepatitis associated with glyburide. Dig Dis Sci 1996;41:322-5. Back to cited text no. 31 [PUBMED] |
| 32. | Ananth JV, Ban TA, Lehmann HE. Tolbutamide jundice associated with multiple drug therapy.Can Med Assoc J 1970;103:1194. Back to cited text no. 32 [PUBMED] |
| 33. | Nakao NL, Gelb AM, Stenger RJ, Siegel JH. A case of chronic liver disease due to tolazamide . Gastroenterol 1985;89:192-5. Back to cited text no. 33 |
| 34. | Bridges ME, Pittman FE. Tolazamide-induced cholestasis. South Med J 1980;73:1072-4. Back to cited text no. 34 |
| 35. | Babich MM, Pike I, Shiffman ML. Metformin-induced acute hepatitis. Am J Med 1998;104:490-2. Back to cited text no. 35 |
| 36. | Deutsch M, Kountouras D, Dourakis SP. Metformin hepatotoxicity. Ann Intern Med 2004;140:25. Back to cited text no. 36 |
| 37. | Nammour FE, Fayad NF, Peikin SR. Metformin-induced cholestatic hepatitis. Endocr Pract 2003;9:307-9. Back to cited text no. 37 |
| 38. | Neuschwander-Tetri BA, Brunt EM, Wehmeier KR, Sponseller CA, Hampton K, Bacon BR. Interim results of a pilot study demonstrating the early effects of the PPAR-gamma ligand rosiglitazone on insulin sensitivity, aminotransferases, hepatic steatosis and body weight in patients with non-alcoholic steatohepatitis. J Hepatol 2003;38:434-40. Back to cited text no. 38 |
| 39. | Graham DJ, Green L, Senior JR, Nourjah P. Troglitazone-induced liver failure: a case study. Am J Med 2003;114:299-306. Back to cited text no. 39 |
| 40. | May LD, Lefkowitch JH, Kram MT, Rubin DE. Mixed hepatocellular-cholestatic liver injury after pioglitazone therapy. Ann Intern Med 2002;136:449-52. Back to cited text no. 40 |
| 41. | Dhawan M, Agrawal R, Ravi J, Gulati S, Silverman J, Nathan G, et al . Rosiglitazone-induced granulomatous hepatitis. J Clin Gastroenterol 2002;34: 582-4. Back to cited text no. 41 |
| 42. | Forman LM, Simmons DA, Diamond RH. Hepatic failure in a patient taking rosiglitazone. Ann Intern Med 2000;132:118-21. Back to cited text no. 42 |
| 43. | Madonia S, Pietrosi G, Pagliaro L. Acarbose-induced liver injury in an anti-hepatitis C virus positive patient. Dig Liver Dis 2001;33:615-6. Back to cited text no. 43 |
| 44. | Tomita K, Azuma T, Kitamura N, Nishida J, Tamiya G, Oka A, et al . Pioglitazone prevents alcohol-induced fatty liver in rats through up-regulation of c-Met. Gastroenterol 2004;126:873-85. Back to cited text no. 44 |
| 45. | Galli A, Crabb DW, Ceni E, Salzano R, Mello T, Svegliati-Baroni G, et al . Antidiabetic thiazolidinediones inhibit collagen synthesis and hepatic stellate cell activation in vivo and in vitro . Gastroenterol 2002;122:1924-40. Back to cited text no. 45 |
| 46. | Lahoti S, Lee WM. Hepatotoxicity of anticholesterol, cardiovascular, and endocrine drugs and hormonal agents. Gastroenterol Clin North Am 1995;24: 907-22. Back to cited text no. 46 |
| 47. | Garovic VD. Hypertension in pregnancy: Diagnosis and treatment. Mayo Clin Proc 2000;75:1071-6. Back to cited text no. 47 |
| 48. | Stravitz RT, Sanyal AJ. Drug-induced steatohepatitis. Clin Liver Dis 2003;7: 435-51. Back to cited text no. 48 |
| 49. | Lafuente NG Calcium channel blockers and hepatotoxicity. Am J Gastroenterol 2000;95:2145. Back to cited text no. 49 |
| 50. | Tabak F, Mert A, Ozaras R, Biyikli M, Ozturk R, Ozbay G, et al . Losartan-induced hepatic injury. J Clin Gastroenterol 2002;34:585-6. Back to cited text no. 50 |
| 51. | Gonzalez-Jimenez D, Varela JM, Calderon E, Galindo J, Gonzalez de la Puente MA. Candesartan and acute liver injury. Eur J Clin Pharmacol 2000;56: 769-70. Back to cited text no. 51 |
| 52. | Kiykim A, Altintas E, Sezgin O, Sezer K, Tiftik N, Akbay E, et al . Valsartan-induced hepatotoxicity in a HBs-Ag-Positive patient. Am J Gastroenterol 2003;98:507. Back to cited text no. 52 |
| 53. | Bas V, Erkan T, Caliskan S, Sever L, Kasapcopur O, Ozbay G, et al . Toxic hepatitis due to enalapril in childhood. Pediatr Int 2003;45:755-7. Back to cited text no. 53 |
| 54. | Thomas LA, Cardwell MS. Acute reactive hepatitis in pregnancy induced by alpha-methyldopa. Obstet Gynecol 1997;90:658-9. Back to cited text no. 54 |
| 55. | Tameda Y, Hamada M, Takase K, Nakano T, Kosaka Y. Fulminant hepatic failure caused by ecarazine hydrochloride (a hydralazine derivative). Hepatol 1996; 23:465-70. Back to cited text no. 55 |
| 56. | Hagmeyer KO, Stein J. Hepatotoxicity associated with carvedilol. Ann Pharmacother 2001;35:1364-6. Back to cited text no. 56 |
| 57. | Pessayre D, Bichara M, Degott C, Potet F, Benhamou JP, Feldmann G. Perhexiline maleate-induced cirrhosis. Gastroenterol 1979;76:170-7. Back to cited text no. 57 |
| 58. | McGovern B, Garan H, Kelly E, Ruskin JN. Adverse reactions during treatment with amiodarone hydrochloride. Br Med J 1983;287:175-80. Back to cited text no. 58 |
| 59. | Fogoros RN, Anderson KP, Winkle RA, Swerdlow CD, Mason JW. Amiodarone: clinical efficacy and toxicity in 96 patients with recurrent, drug-refractory arrhythmias. Circulation 1983;68:88-94. Back to cited text no. 59 |
| 60. | Mason JW. Amiodarone. N Eng J Med 1987;316:455-66. Back to cited text no. 60 |
| 61. | Chang CC, Petrelli M, Tomashefski JF Jr, McCullough AJ. Severe intrahepatic cholestasis caused by amiodarone toxicity after withdrawal of the drug: a case report and review of the literature. Arch Pathol Lab Med 1999;123:251-6. Back to cited text no. 61 |
| 62. | Moffat DF, Oien KA, Dickson J, Habeshaw T, McLellan DR. Hepatocellular carcinoma after long-term tamoxifen therapy. Ann Oncol 2000;11:1195-6. Back to cited text no. 62 |
| 63. | Smith LL, Brown K, Carthew P, Lim CK, Martin EA, Styles J, et al . Chemoprevention of breast cancer by tamoxifen: risks and opportunities. Crit Rev Toxicol 2000;30:571-94. Back to cited text no. 63 |
| 64. | Storen EC, Hay JE, Kaur J, Zahasky K, Hartmann L. Tamoxifen-induced submassive hepatic necrosis. Cancer J 2000;6:58-60. Back to cited text no. 64 |
| 65. | Murata Y, Ogawa Y, Saibara T, Nishioka A, Fujiwara Y, Fukumoto M, et al . Unrecognized hepatic steatosis and non-alcoholic steatohepatitis in adjuvant tamoxifen for breast cancer patients. Oncol Rep 2000;7:1299-304. Back to cited text no. 65 |
| 66. | Lee KS, Buck M, Houglum K, Chojkier M. Activation of hepatic stellate cells by TGF alpha and collagen type I is mediated by oxidative stress through c-myb expression. J Clin Invest 1995;96:2461-8. Back to cited text no. 66 |
| 67. | Morgan MY, Reshef R, Shah RR, Oates NS, Smith RL, Sherlock S. Impaired oxidation of debrisoquine in patients with perhexiline liver injury. Gut 1984;25: 1057-64. Back to cited text no. 67 |
| 68. | Berson A, De Beco V, Letteron P, Robin MA, Moreau C, El Kahwaji J, et al . Steatohepatitis-inducing drugs cause mitochondrial dysfunction and lipid peroxidation in rat hepatocytes. Gastroenterol 1998;114:764-74. Back to cited text no. 68 |
| 69. | Pessayre D, Berson A, Fromenty B, Mansouri A. Mitochondria in steatohepatitis. Semin Liver Dis 2001;21:57-69. Back to cited text no. 69 |
| 70. | Chitturi S, Farrell GC. Etiopathogenesis of nonalcoholic steatohepatitis. Semin Liver Dis 2001;21:27-41. Back to cited text no. 70 |
| 71. | Robertson G, Leclercq I, Farrell GC. Nonalcoholic steatosis and steatohepatitis. II. Cytochrome P-450 enzymes and oxidative stress. Am J Physiol Gastrointest Liver Physiol 2001;281:1135-9. Back to cited text no. 71 |
| 72. | Rao MS, Reddy JK. Peroxisomal beta-oxidation and steatohepatitis. Semin Liver Dis 2001;21:43-55. Back to cited text no. 72 |
| 73. | Bedoucha M, Atzpodien E, Boelsterli UA. Diabetic KKAy mice exhibit increased hepatic PPARγamma1 gene expression and develop hepatic steatosis upon chronic treatment with antidiabetic thiazolidinediones . J Hepatol 200l;35:17-23. Back to cited text no. 73 |
| 74. | Zimmerman HJ, Ishak KG. General aspects of drug-induced liver disease. Gastroenterol Clin North Am 1995;24:739-57. Back to cited text no. 74 |
Copyright 2006 - Indian Journal of Pharmacology
The following images related to this document are available:
Photo images
[ph06066t3.jpg]
[ph06066t2.jpg]
[ph06066t1.jpg]
|

![[Table - 1]](/showimage?ph/photo/ph06066t1.jpg){kind=link}
{kind=link}
![[Table - 3]](/showimage?ph/photo/ph06066t3.jpg){kind=link}