 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
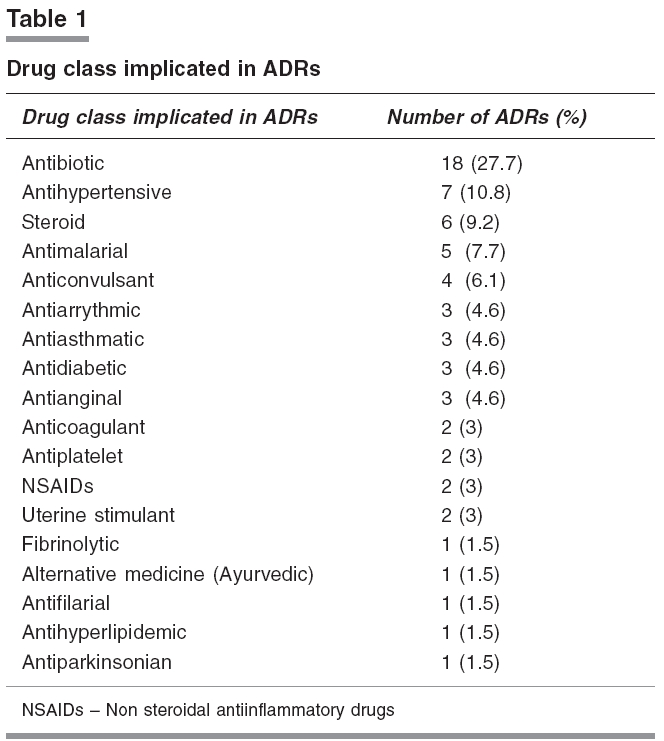
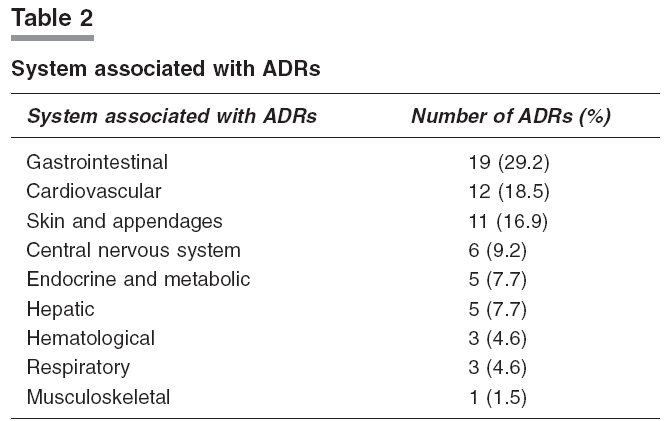
Indian Journal of Pharmacology, Vol. 38, No. 4, July-August, 2006, pp. 293-294 Research Letter Implementation and results of an adverse drug reaction reporting programme at an Indian teaching hospital Rao PadmaG.M, Archana B, Jose J Department of Pharmacy Practice, Manipal College of Pharmaceutical Sciences, Manipal Academy of Higher Education, Manipal Code Number: ph06079 Adverse drug reactions (ADRs) are negative consequences of drug therapy.[1] At least one ADR has been reported to occur in 10 to 20% of hospitalised patients.[2] In the recent past, pharmacists and pharmacologists have been encouraged to participate in and contribute to the ADR monitoring and reporting programmes in different parts of the world. ADR monitoring and reporting activity is in its infancy in India. ADR reporting programmes on an institutional basis can support the setting up of a sound pharmacovigilance system in the country. Furthermore, productive hospital-based ADR programmes can provide valuable information about potential problems in drug usage in an institution. Dr. T.M.A. Pai hospital, Udupi is a 200-bed teaching hospital and is a constituent of Kasturba Hospital (KH), Manipal (a tertiary care hospital). The department of pharmacy practice has been carrying out an ADR reporting programme at KH from July 2001. Dr. T.M.A. Pai hospital did not have such a system. Therefore, the present study was undertaken with the objective of initiating a similar system at the hospital to study the incidence and the pattern of ADRs occurring in this hospital. This was a spontaneous reporting study conducted for a period of seven months (October 2003- April 2004) and coordinated by clinical pharmacists. Various methods were adopted to create awareness about ADR reporting system. These included ADR reporting awareness posters and personal interaction with health care professionals. Health care professionals were encouraged to report all suspected ADRs through various modes, which included reporting through ADR reporting forms available at all the nursing stations and out-patient departments, telephonic reporting, and direct reporting to the clinical pharmacist who attended ward rounds in various departments on rotation basis. After the intimation of suspected ADR, additional details were collected for further assessment of the ADR by the clinical pharmacist. In the present study, only the reports of ADRs in the inpatients were evaluated. The incidence and pattern of ADRs were evaluated. Further, the individual ADR reports were assessed to find out whether the ADR was the reason for the present admission of the patient to the hospital. All reported ADRs were evaluated for the following parameters using appropriate scale. 1) Causality (Naranjo's algorithm)[3] A total of 1821 patients were admitted in the hospital, and 65 ADRs were reported from 51 patients during the seven-month study period. At least one ADR was reported in 2.8% of hospitalised patients. Among the reported ADRs, in six cases the ADR was the sole reason or one of the reasons which contributed to the hospitalisation of the patient. Out of the 65 ADRs reported, 42 (64.6%) were identified and reported by physicians and nurses, while the remaining 23 (35.4%) were identified and reported by the clinical pharmacist. Majority of the reports were from the medicine department (84.6%), followed by pediatrics (10.8%), OBG (3%) and orthopedics (1.5%). In terms of the patient demographics in the reported ADRs, 32 were females and 19 were males. Number of patients in pediatric (0-18 years), adult (19-60 years), and geriatric (>60 years) groups were 6, 27, and 18, respectively. Drug class implicated in the ADR reports and the system affected by the reactions are represented in [Table - 1],[Table - 2], respectively. Upon causality assessment it was found that most of the ADRs belonged to the category possible (52.3%), followed by probable (46.2%) and unlikely (1.5%). Of the reported ADRs, 64.6% were moderate in severity, 29.2% were mild, and 6% were severe. Most of the ADRs (52.3%) were managed by symptomatic treatment, while 4.6% cases required specific treatment. The incidence of ADRs observed in this study was found to be low compared with the incidence mentioned by Murphy et al [5] based on the data from other studies. According to Murphy et al as many as 35% of hospitalised patients experienced an ADR during their hospital stay. One major reason for this could be underreporting, similar to that observed in another Indian study.[6] Out of the 92 health care professionals who were working in the hospital during our seven-month study period, only 14 (15.2%) reported at least one ADR. The concept of such a reporting system was new to the health care professionals, which might have contributed to underreporting. Underreporting, a major draw back of spontaneous ADR reporting, is prevalent even in developed countries with a long history of functional ADR reporting system. A method that could be employed to tackle this problem in a hospital set-up is to increase awareness about an existing system and the advantages of ADR reporting. Furthermore, provision of 'thank you' note to the reporters along with additional details that could be educational in nature, on the reported ADR, could help in motivating them for future reporting. Periodic dissemination of data on the reported ADRs to the health care professionals would provide information to them on the pattern of ADRs occurring in the local population. These are some of the methods that could probably improve compliance with spontaneous ADR reporting among the health care professionals. Antibiotics were the most commonly implicated drug class, a finding consistent with other studies.[5],[7],[8] Among the various systems affected by ADRs, gastrointestinal system was the one most commonly associated with ADRs, and this finding is consistent with the reports of an Indian study.[6] The causality assessment revealed that most of the ADRs belonged to "possible" followed by "probable" categories, similar to that reported by Murphy et al . [5] Severity assessment showed highest percentage of moderate reactions, a finding consistent with the study carried out by Ramesh et al [6] and Gholami et al . [1] This study was useful as a preliminary study in initiating a culture of ADR reporting among health care professionals in the hospital under study. Reporting programmes are necessary to educate and to increase awareness about reporting of ADRs among the healthcare professionals in the developing countries. Furthermore, these programmes help to obtain information on the incidence and the pattern of ADRs in the local population. References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06079t2.jpg] [ph06079t1.jpg] |
| |||||||||

{kind=link}
{kind=link}