 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
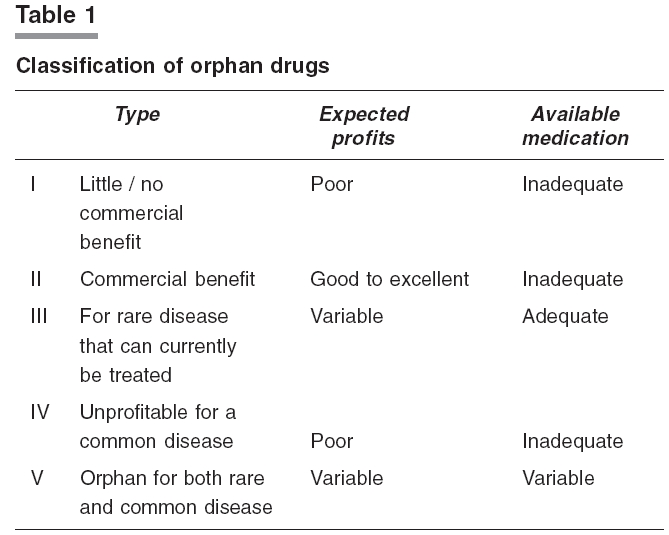
Indian Journal of Pharmacology, Vol. 38, No. 4, July-August, 2006, pp. 299-300 Correspondence Orphan diseases and drugs Badyal D Department of Pharmacology, Christian Medical College, Ludhiana-141 008 Code Number: ph06083 Related articles: ph06042, ph06082 We read with interest the topic on "orphan disease and drugs" (Ind J Pharmacol 2006; 38: 171-76). The author has appropriately highlighted the need for orphan drug regulation. We feel that there should have been more information on basic and important issues associated with orphan diseases and drugs, which are more relevant clinically. These issues which should have been discussed in detail are (1) debatable definition, (2)classifying orphan drugs for industry and physicians and (3) third world countries and research and development of orphan drugs. 1. It is not as simple as it looks to define orphan drugs. The author referred to as orphan drugs, which are intended to treat diseases affecting a small number of patients. Regulatory and economic developments now force consideration of much broader definition. In more recent times, the definition has been broadened to include drugs for diseases endemic in third world countries where number of patients may be sufficient but purchase and distribution of effective drugs may be impossible for improvised population. Hence orphan drugs can be defined as "those drugs intended to treat either a rare disease or a more common disease where manufacturer cannot expect to make profits".[1] For example, drugs and vaccine for tropical diseases are also defined as orphan drugs because patient sufferings from these diseases, although numbering tens of millions, are too poor to pay the price of medications. Vaccines are virtual orphans and also called economic orphans. The number of vaccines introduced in the market has decreased drastically in the recent years.[2] In a few special cases the term orphan drug may have to be redefined. Earlier the growth hormone (GH) was obtained from cadavers, but nowadays it is manufactured by recombinant technology. The patient population in USA which may use recombinant GH is not large but this number must be multiplied by the cost per year per patient. In spite of profitable market, the hormone is still classified as orphan drug.[3] A large number of recombinant protein drugs coming into market, need appropriate classification. 2. Orphan drugs available to treat rare diseases are a heterogenous group. Earlier classifications of orphan drugs divided these drugs into four general categories or 18 separate detailed categories based on the stage of development. [Table - 1] represents a classification of five categories of orphan drugs based on their commercial potential and the availability of adequate treatment. This classification is close to the way in which regulators have defined and described orphan drugs than the earlier classifications. Pharmaceutical industries consider both the stage of development as well as commercial and medical potential when describing or classifying orphan drugs. So, all the classification is relevant for the pharmaceutical industry. Practising physicians think in terms of drug's availability to the patient use, and thus former two classifications are more important to them than the last one. Drugs can shift from one category to other. A number of drugs have crossed from the type1 to type III categories over previous few years. These include Wilson's disease, which can now be treated with penicillamine, zinc and triethylenetetramine and rare bacterial diseases that can be treated with antimicrobials. Type I and III orphan drugs are usually the most difficult ones to find sponsors for if the drugs are known to have activity but are yet not marketed. These drugs can become profitable type V drugs if these drugs are found to be effective in treating a common disease.[4] 3. The issue of orphan drugs becomes more important for third world countries like India, which are affected the most. Why no new drug is coming up or nobody is investing in research and development (R&D) in malaria, leishmania etc. Usually we criticize the pharmaceutical industry or manufacturers for this. This is a controversial issue. The manufacturers cannot be entirely blamed for this. It is not easy to produce and market orphan drugs. The manufacturers of drugs have to amortize their operational expenses, their research investment and they have to make reasonable profit so that they can finance new ventures in the future. It is calculated that return on investment for the average new chemical entity (NCE) is barely 6-8%, a figure with serious implications for a prudent businessman.[5] One area where the orphan drug act (ODA) has not provided very strong incentives is new drugs and vaccines for the neglected diseases such as malaria and tuberculosis that affect poor countries. Given their low prevalence in the United States, diseases that predominantly affect poor countries are technically eligible for all of the incentive provisions of the ODA. However, developing countries lack the resources to afford these drugs, with many devoting as little as $2 per capita per year to heath care. Also R&D costs have been rising and drug prices declining.[6] Hence these figures too suggest a flow from less attractive to more attractive alternatives for investment. But what if most of the drugs failed to be developed for the lack of R&D investment! Are economic implications more important than medical ones or vice versa ? A country should try to produce important drugs for the benefit of the whole world, depending on the R&D investment, the return on such investment, the tax and patent incentives and its regulatory policies. Agreement of these points might lead to beneficial changes in our national thinking and prevent "orphanisation of new drugs". References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06083t1.jpg] |
| |||||||||

{kind=link}