 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
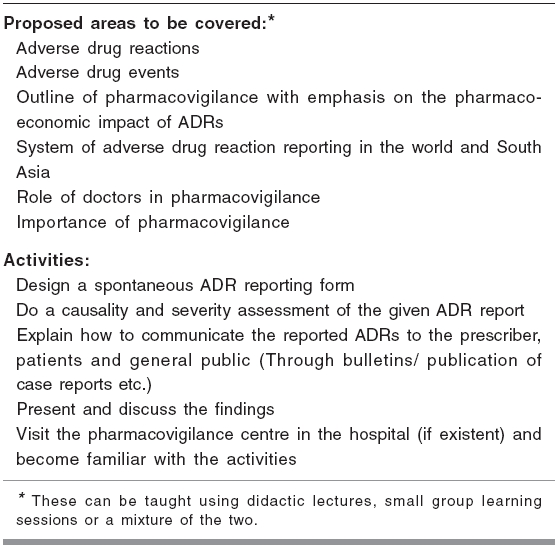
Indian Journal of Pharmacology, Vol. 38, No. 5, September-October, 2006, pp. 316-319 Education Forum Teaching pharmacovigilance to medical students and doctors Shankar PRavi, Subish P, Mishra P, Dubey AK Department of Pharmacology, Manipal College of Medical Sciences, Pokhara Date of Submission: 03-Dec-2005 Code Number: ph06091 Abstract The World Health Organisation defines pharmacovigilance as 'the pharmacological science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other drug-related problem'. Pharmacovigilance plays an important role in ensuring drug safety. Hence,every country needs a functioning pharmacovigilance programme. Pharmacovigilance is being taught, in theory, in many developed countries, but the practical approach is missing in developing countries. Pharmacovigilance should ideally be taught to small groups of medical students, interns, postgraduates and practitioners by linking it to the activities of a functioning pharmacovigilance centre in a teaching hospital. It should be activity-based, problem-based and linked to the rational use of medicines. Students should be trained during their internship and residency. The non-inclusion of pharmacovigilance in university syllabi and unfamiliarity with problem-based learning could prove to be stumbling blocks to the success of the concept. Pharmacologists should create awareness on pharmacovigilance among doctors of other specialities and enlist their support in teaching the subject. Keywords: Adverse effects, ADR monitoring, post-marketing surveillance, teaching-learning. Introduction The World Health Organisation (WHO) defines pharmacovigilance as 'the science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other drug-related problems'.[1] Pharmacovigilance is concerned with the post-marketing surveillance of medicines and the use of the information generated for education and effective drug regulation.[2]Adverse drug reactions and adverse drug events An adverse drug reaction (ADR) is 'a response to a medicine which is noxious and unintended, and which occurs at doses normally used in man'.[3] Karch and Lasagna define ADR as 'any response to a drug that is noxious and unintended and that occurs at doses used in man for prophylaxis, diagnosis or therapy, excluding failure to accomplish the intended purpose'.[4] An adverse drug event (ADE) is 'any untoward medical occurrence that may present during treatment with a medicine, but which does not necessarily have a causal relationship with the treatment'.[3]Benefits of pharmacovigilance Pharmacovigilance plays an important role in the rational use of medicines by providing information about ADRs in the general population. Knowledge of the adverse effects of drugs is important for effective treatment. Communicating the potential harm of drug-use to patients is a matter of high priority and should be carried out by every prescriber.[1] Information collected during the pre-marketing phase of drug development may not detect rare ADRs. The use of a drug during a clinical trial is under controlled conditions. Clinical trials generally enroll a selected, limited number of patients[3] and may not include certain sections of the population. Drug use in special situations or drug interactions may not be studied.[3] Therefore, the post-marketing surveillance of drugs is important. Every country needs to have its own pharmacovigilance programme due to differences in the pattern, presentation and incidence of ADRs. There may be differences in diseases and prescribing practices, genetic composition of the population, diet and traditions of the people. There could also be differences in drug manufacturing processes, drug distribution and use. Traditional and complementary drugs may be used along with modern allopathic medicines. Data derived from within a country has relevance for that particular population and may be helpful for rational regulatory decision-making.[3] The development of a better system of reporting ADRs has been recommended as a top priority action to prevent ADRs and ADEs in hospitals.[5] Present status of teaching pharmacovigilance in medical institutions In the United Kingdom (UK), 57% of medical schools assessed student knowledge of the Yellow card scheme (the system of spontaneous reporting in the UK) and the scheme featured in the majority of undergraduate syllabi.[6] In France, a systematic collection of ADRs, over a period of nearly 20 years, resulted in increased information about recent drugs and new and/or not well-known ADRs, which helped to educate doctors on the rational prescription of drugs and pharmacovigilance.[7]Present knowledge of pharmacovigilance among medical students and practitioners A study in a medical college in New Delhi found that the knowledge, attitudes and practices (KAP) regarding ADR monitoring was comparable among undergraduates and prescribers, but overall the scores needed improvement.[8] A survey among medical residents in France showed that the majority lacked knowledge of pharmacovigilance.[9] In a northern Italian district, it was observed that doctors had little information on ADRs and their reporting systems.[10]Advantages of teaching pharmacovigilance to medical students Spontaneous ADR reporting, during post-marketing surveillance, has been shown to detect adverse event signals resulting from drug use in the population.[11] In an effective surveillance programme, under reporting should be low and there should be active participation by the clinicians and other healthcare workers. The quality of reports generated depends on the knowledge and training of the clinicians.[11] Teaching pharmacovigilance to medical students makes them realise that all medicines can cause ADRs. It emphasises their responsibility to participate in the national pharmaco-vigilance system.[2] Spontaneous reporting schemes have been a major source of information in pharmacovigilance. The knowledge of drug safety issues can improve the manner in which a doctor takes the clinical history of a patient, with more emphasis on the medication history, and can help to understand the behaviour of drugs better. It can decrease the irrational use of medicines, adverse drug-drug interactions and inappropriate polypharmacy. Teaching pharmacovigilance to medical students Pharmacovigilance can be taught during the undergraduate course. Pharmacovigilance modules must be linked to modules on the rational use of medicines (RUM). The Uppsala Monitoring Centre (UMC), the international collaborating centre for ADR monitoring, has suggested a number of basic components of a pharmacovigilance course for pharmacologists and other healthcare personnel.[2]Objectives of a pharmacovigilance teaching programme An outline of ADRs is covered in most undergraduate pharmacology textbooks and curricula. Though the present academic curricula mention ADRs, they do not train students to apply pharmacovigilance in their future practice. The objective of the programme should be to create awareness on pharmacovigilance among medical students. In their future practice, they should be able to report ADRs using the spontaneous ADR reporting form. They need to be aware of the reporting system in their area or region.Content of the teaching programme The content of the proposed pharmacovigilance programme is outlined in [Table - 1]. The information (theory) is to be covered in two lectures (preferably, small group briefings) of 1 h duration each. The first two activities (designing a reporting form and carrying out a severity and causality assessment of the given ADR report) can be done in a problem-based learning/problem-stimulated learning (PBL/PSL) session, of 2½ h duration. The visit to the pharmacovigilance centre and the presentation and discussion of findings can be done in the second session. A total of 6-7 h may be required, but colleges can modify the time component according to their requirements. However, a minimum of 6 h should be spent on pharmacovigilance.Teaching-Learning methods Lectures can be organised on the aims and need for pharmacovigilance and the practice of spontaneous reporting. The organisational set-up of the pharmacovigilance programme in particular regions and in the country should be highlighted. After a preliminary introduction, all further learning should be activity-based and carried out in small groups.Evaluation methods With respect to [Table - 1], the theoritcal aspect can be assessed using short answer type questions and multiple choice questions (MCQs). Designing the ADR reporting form is a group activity and formative assessment is the best option. Causality and severity assessment of the ADR can be done through objective structured practical examination (OSPE). ADR briefing (detection, reporting, initial management and prevention) to a patient can be assessed at an OSPE station, using a standardised checklist.Teaching and learning pharmacovigilance at our institution Our institution (Manipal College of Medical Sciences, Pokhara) has a regional pharmacovigilance centre and a drug information centre (DIC). Currently, we concentrate on the spontaneous reporting of ADRs by clinicians and other healthcare personnel. In Nepal, pharmacology is taught in the first 4 semesters of the MBBS course, in an integrated manner, with the other basic science subjects. The basic principles of pharmacovigilance are detailed and the students are instructed to design a spontaneous ADR reporting form. They are given reports of ADRs from the pharmacovigilance centre and instructed to conduct the causality assessment of the ADR, using the Naranjo algorithm,[12] and the severity assessment, using the modified Hartwig scale.[13] They visit the DIC and the pharmacovigilance centre to understand the reporting system in the hospital. Currently, our students are taught the process of pharmacovigilance reporting in Nepal. The role of the physician in ADR reporting and the importance of co-operation with other healthcare professionals are emphasised. Some of our students have reported ADRs to the pharmacovigilance centre during their clinical training. Student feedback on the activity-based learning sessions has been positive. Our students have found the sessions educative, informative and interesting. They have said that designing a spontaneous ADR reporting form sensitized them to the importance of reporting ADRs.[14] Student knowledge about pharmacovigilance, assessed during informal discussions and viva voce , was found to be satisfactory. We are working on an assessment framework for the other activities which were carried out. Pharmacovigilance training during internship Interns and medical officers (MOs) can play a key role in reporting ADRs. Teaching and training programmes should be conducted to sensitise them to the importance of reporting ADRs. Details about the ADR reporting programme in particular hospitals and regions should be provided. Young doctors should be taught how to report ADRs to the centre concerned, using the ADR reporting form. Methods for assessing the causality, severity and preventability of ADRs should be highlighted. The importance of preventing ADRs, if possible should be covered. Pharmacovigilance training should be linked to training sessions on RUM. In our hospital, no formal training programmes for interns and MOs exist. However, we emphasise the importance of reporting ADRs whenever interns and MOs visit the DIC. Plans are afoot to start sessions on RUM (including pharmacovigilance) in the near future. Possible problems while teaching pharmacovigilance Teaching the basics of pharmacovigilance to medical students may require 2 h of lectures/briefing sessions and 4-5 h of activity-based learning. Allotting time for pharmacovigilance in a busy undergraduate curriculum may be difficult. In our institution, the teaching-learning sessions are spread over the first 4 semesters. The syllabi of most universities do not specify pharmacovigilance as a subject. Teachers may be reluctant to teach and students may be reluctant to learn a subject which is not in the syllabus. Teaching pharmacovigilance is relatively easy if there is a functioning centre in the institution which students can visit. Pharmacovigilance training can be linked to pre-existing sessions on RUM. The lack of knowledge among medical teachers on pharmacovigilance and RUM can be addressed by formulating training programmes. The co-operation of clinical teachers is essential in teaching pharmacovigilance. Pharmacovigilance and RUM can best be taught to small groups, using problem-based and activity-based learning strategies. Knowledge of problem-based strategies among medical teachers would be helpful in this direction. Role of pharmacologists in teaching pharmacovigilance Pharmacologists and pharmacists play an important role in initiating and conducting a pharmacovigilance programme.[15],[16] They can sensitise clinicians by highlighting the importance of pharmacovigilance and by helping them apply its principles in daily practice. Clinicians, who practise pharmacovigilance, are important allies in teaching the subject to medical students.Teaching pharmacovigilance to postgraduate students All postgraduate (PG) students of pharmacology (MD, MSc) should have a thorough knowledge of pharmaco-vigilance. They should be active members of pharmaco-vigilance programmes in their medical colleges or teaching hospitals. In our institution, MSc students play an active role in the programme. The UMC's training programme is a good starting point.[2] PG students, in other specialities, should also be made aware of pharmacovigilance, the need for and importance of reporting ADRs and the reporting procedure. They should be sensitised to ADR reporting during their residency training, with the help of the pharmacology PGs, if necessary. These residents, in turn, can sensitise interns, undergraduate students and other healthcare professionals to the importance of pharmacovigilance.Educating doctors in the community about pharmacovigilance Doctors (general practitioners and specialists) are important in reporting ADRs to the pharmacovigilance programme. Educated doctors in the community will increase the effectiveness of the reporting programme. Pharmacologists have an important role in creating awareness among doctors working in the community. Training programmes for doctors should be problem-based, activity-based and carried out in small groups. In Wales, a distance-learning programme in pharmacovigilance, linked to educational credits, was found to significantly improve the rate and quality of ADR reporting by general practitioners and pharmacists.[17]Conclusion Pharmacovigilance is important to esnure the safe use of medicines. Teaching pharmacovigilance to medical students will make them aware of their responsibility to report ADRs. The teaching should be mainly problem-based, activity-based and carried out in small groups. MOs and interns should be made aware of reporting systems in their hospitals. Doctors, from other specialities, have an important role in reporting ADRs and sensitising medical students to the importance of pharmacovigilance. Pharmacologists have the primary responsibility of running a pharmacovigilance programme. Postgraduate pharmacology students should be actively involved in the running of a pharmacovigilance centre.References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06091t1.jpg] |
| |||||||||

{kind=link}