 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
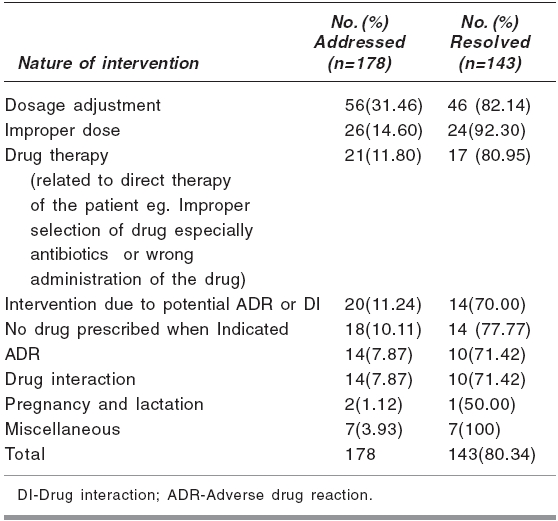
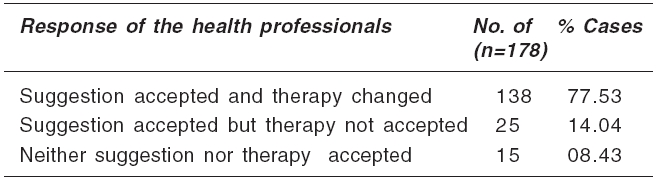
Indian Journal of Pharmacology, Vol. 38, No. 5, September-October, 2006, pp. 361-362 Research Letter Clinical interventions: A preliminary survey in a South Indian teaching hospital Mangasuli S, Rao PadmaGM Department of Pharmacy Practice, 4th Floor, Shirdi Sai Baba Cancer Hospital,Manipal-576104, Karnataka Code Number: ph06101 Though pharmacy practice has changed significantly in recent years and continues to evolve towards the provision of better pharmaceutical care, pharmacists represent an under-utilised but potential resource to optimize the usage of drugs. Studies have shown that a clinical pharmacist can reduce health service use and costs while improving the appropriateness of drug prescribing.[1],[2],[3] Medication errors most often occur due to insufficient information and time during prescription. The present study was carried out by the Department of Pharmacy Practice, established in July 2001 at Kasturba Hospital, a tertiary care teaching hospital in Manipal, India. The objective was to survey clinical interventions by clinical pharmacists, and their acceptance by clinicians. A standard format was designed to collect relevant data for each intervention such as brief details of the patient, medications, problem identified, physician's response and follow up, if any. Intervention for study purpose was defined as an action by a pharmacist which resulted in a change in the patient's therapeutic management. Clinical pharmacists routinely monitored patients' drug therapy and interviewed them, when necessary. Any drug-related problem was identified and discussed during the ward rounds with the physicians concerned. A drug related problem can be defined as any event or circumstance involving the drug treatment, which interferes or potentially interferes with the patient, achieving an optimum outcome of medical care. Eight categories of drug related problems are identified by Hepler CD and Strand LM in 1990.[4] They are: a) untreated indication, b) inappropriate drug selection, c) sub-therapeutic dose d) overdosage, e) adverse drug reaction f) failure to receive the drug, g) drug interaction and h) drug use without indication. All the interventions, over a period of 3 years between July 2001 and December 2004, were evaluated for their appropriateness. Out of 188 interventions, 178 were analysable. The remaining could not be analysed due to incompleteness. Also, all the interventions were done on in-patients, due to limited pharmacist manpower. For the same reason, pharmacists were recruited in speciality wards and neurology, nephrology and PTCD (pulmonary, thorax and chest department) on a project basis only. The pharmacist:patient ratio was on an average of 1:20 in 7 medicine units and all speciality units. All the pharmacists were either full-time faculty members or postgraduate students in clinical pharmacy. There were only 2 (1.13%) interventions observed between July 2001 and December 2002. Nevertheless, there was a constant upsurge observed in the number of clinical interventions in 2002, 2003 and 2004, i.e. 28 (15.73%), 62 (34.83%) and 87 (48.88%) respectively. Most of the interventions (171) were done in general medicine wards (96.1%). The remaining were done in cardiology 3 (1.69%), PTCD 1 (0.56%), neurology 2 (1.12%), nephrology 1 (0.56%). The various categories of drug related problems identified by clinical pharmacists and the responses of the health care professionals to these clinical interventions, during the above period, are listed in [Table - 1][Table - 2]. Out of the 178 interventions analysed, the interventions by pharmacists were accepted and the prescriptions altered accordingly in 139 cases (78.1%). There were 20 (11.2%) other interventions where suggestions were accepted, but therapy was not changed either because the physicians were hesitant to change the prescription immediately, without close monitoring, or because the suggestions were thought to be insignificant. In 15 (8.4%) cases, the suggestions were neither accepted nor therapy changed. One of the reasons for this could be that the pharmacists failed to understand the sophisticated prescribing behaviour i.e., prescribing decisions governed by clinical experience of physicians For instance, a patient, with Type 2 DM and hyperlipidaemia, on insulin and capsule fenofibrate, complained of myalgia. The pharmacist suspected fenofibrate-induced myotoxicity and suggested a test for creatin kinase levels, while the physician believed that the pain was neuropathic in nature, not muscular, so, it was unlikely to be related to fenofibrate. The most common drug-related problem (31.46%) was that patients' dosage adjustments were not based on renal and hepatic status. Improper dosage administration ranked second in the intervention category (14.60%), followed by drug therapy (11.80%) related interventions such as improper selection of the drug in the case of antibiotics, improper time of administration of the drug to reduce CNS symptoms and so on. Interventions were also done when there was a possibility of ADR or drug interaction (11.24%) due to predisposing factors. [Table - 1] The guidelines followed for drug therapy monitoring (DTM) in patients are 'Practice, Standards and Definitions' by the Society of Hospital Pharmacists of Australia (as we don't have any Indian guidelines) for clinical pharmacy services such as medication history interviews of patients, drug therapy monitoring which includes medication order review, adverse drug reaction management, therapeutic drug monitoring and so on. Interventions related to identification of ADRs were observed in 14 (7.87%) cases, followed by pregnancy and lactation related interventions in 2 (1.12%) cases. Miscellaneous errors (3.93%) included doctors not prescribing drugs which the patient needed or prescribing drugs which the patient did not need. There were instances when medication was prescribed by the physician, but the treatment chart was not updated and the omission error was detected by the pharmacist. Over 10% of the interventions was deemed to have reduced the probability of re-admission of the patient due to potential ADR and drug interaction. Similarly, cases, where dosage was sub-optimal, over-dosage or presence of indication but no medication would have either caused treatment failure, disease relapse or prolonged hospital stay, were also observed and documented. Therefore, clinical pharmacist interventions can have a positive impact on reducing drug-related errors in overall patient care. Physicians were receptive to the recommendations to resolve drug related problems, suggesting that a joint effort between physicians and pharmacist is possible. Acknowledgments Authors are sincerely thankful to all the faculty members and postgraduate students of Department of Pharmacy Practice, Manipal College of Pharmaceutical Sciences for actively participating in wards rounds and making clinical interventions.References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06101t2.jpg] [ph06101t1.jpg] |
| |||||||||

{kind=link}
{kind=link}